Vygotsky in applied neuropsychology
Abstract
The aims of this paper are: 1) to show the role of clinical experience for the theoretical contributions of L.S. Vygotsky, and 2) to analyze the development of these theories in contemporary applied neuropsychology. An analysis of disturbances of mental functioning is impossible without a systemic approach to the evidence observed. Therefore, medical psychology is fundamental for forming a systemic approach to psychology. The assessment of neurological patients at the neurological hospital of Moscow University permitted L.S. Vygotsky to create, in collaboration with A.R. Luria, the theory of systemic dynamic localization of higher mental functions and their relationship to cultural conditions. In his studies of patients with Parkinson’s disease, Vygotsky also set out 3 steps of systemic development: interpsychological, then extrapsychological, then intrapsychological. L.S. Vygotsky and A.R. Luria in the late 1920s created a program to compensate for the motor subcortical disturbances in Parkinson’s disease (PD) through a cortical (visual) mediation of movements. We propose to distinguish the objective mediating factors — like teaching techniques and modalities — from subjective mediating factors, like the individual’s internal representation of his/her own disease. The cultural-historical approach in contemporary neuropsychology forces neuropsychologists to re-analyze and re-interpret the classic neuropsychological syndromes; to develop new assessment procedures more in accordance with the patient’s conditions of life; and to reconsider the concept of the social brain as a social and cultural determinant and regulator of brain functioning. L.S. Vygotsky and A.R. Luria proved that a defect interferes with a child’s appropriation of his/her culture, but cultural means can help the child overcome the defect. In this way, the cultural-historical approach became, and still is, a methodological basis for remedial education.
Received: 03.08.2016
Accepted: 21.09.2016
Themes: Neuropsychology; 120th anniversary of Lev Vygotsky
PDF: http://psychologyinrussia.com/volumes/pdf/2016_4/psychology_2016_4_6.pdf
Pages: 73-79
DOI: 10.11621/pir.2016.0406
Keywords: psychological theory and clinical practice, Vygotsky and Luria, Parkinson’s disease, mediation, cultural-historical approach
Introduction
L.S. Vygotsky is traditionally associated in psychological science with developing the theoretical foundations of psychology, such as the cultural-historical approach; the biological and social determination of child development; the origins of higher mental functions; the nature of human conscience; communication and generalization; mediation, and so on. The role of clinical practice — studies of pathological cases — in his developing these theories is often underestimated in professional papers analyzing Vygotsky’s contributions. The same is true for the perception of other general psychologists such as A.N. Leontiev (Glozman, 2004).
“The new psychology started from practice, not from theories: pedagogical, developmental psychology, and abnormal development (L.S. Vygotsky); clinical work and twins studies (A.R. Luria); concept formation in schoolchildren (A.N. Leontiev); the psychological bases for the formation of story-telling and intelligence in children (A.V. Zaporozhets); children’s appropriation of simple means (P.Ya. Halperin); the development of memory in schoolchildren (P.I. Zinchenko) — the list could go on and on. These were practical tasks, solved by the group directed by L.S. Vygotsky, and after his death, by A.N. Leontiev and A.R. Luria. They worked hard and happily. Theory was their means, not their purpose” (Zinchenko, 1983, p. 9). These conditions can be explained not only by the fact that the pathology is revealing what is hidden in normal people, but an analysis of disturbances in mental functioning is impossible without a systemic approach to the evidence observed. Therefore, medical psychology is fundamental to forming a systemic approach to psychology.
The aim of this paper is: 1) to show the role of clinical experience for the theoretical contributions of L.S. Vygotsky, and 2) to analyze the development of these theories in contemporary applied neuropsychology.
The 1920s
In 1917, L.S. Vygotsky started work in his native town of Gomel, Byelorussia, assessing and helping children with vision and hearing loss, as well as with mental retardation. He presented this work at the International Conference on the Education of the Deaf in London in 1925 (the only trip abroad Vygotsky ever undertook) (Vygotsky, 1925).
On January 6, 1924, Vygotsky presented his paper “The methods of reflexological and psychological investigation” to the Second All-Russian Congress on Psychoneurology in St. Petersburg (first published in 1982). In this presentation, Vygotsky criticized the reflexological approach because of a “declarative, schematic characterization of reflexological studies of the complex human behavior” (Vygotsky, 1924/1982, p. 43), and for the first time declared the need for a systemic approach to understanding mental functioning: “New tasks need new means… Reflexes don’t exist separately but are a part of complex systems, complicated formations that determine human behavior” (Ibid, p. 49). This presentation deeply influenced A.R. Luria and corresponded to his ideas about the systemic nature of human mental functions. Luria initiated Vygotsky’s transfer from Gomel to Moscow, and obtained a place for him as a researcher at the Psychology Institute of Moscow University (Fig. 1).
Vygotsky continued his work with abnormal children in Moscow, and he created a “Medico-pedagogical center of the Narkompros (Ministry of Education) of the Russian Federation,” which was later transformed into the Research Institute of Defectology (now the Institute of Corrective Pedagogy). The main finding from these studies was “a bifurcation in the course of a child’s behavioral development, into natural-psychological development and cultural-psychological development” (Vygotsky & Luria, 1930, p. 30). It was an application of the cultural-historical approach to developmental psychology.

Figure 1. A photo of the psychologists working at the Institute of Psychology, Moscow, in the late 1920s. Seated in the front row: Luria and Vygotsky (second and third from left, respectively). (Reproduced by courtesy of L. Mecacci)
In addition, starting in 1928, Vygotsky and Luria jointly organized the first laboratory of neuropsychology (25 years before the laboratory of neuropsychology at the Burdenko Institute of Neurosurgery) at the neurological hospital of Moscow University on Rossolimo Street. This laboratory is still in operation. His assessment of neurological patients permitted L.S. Vygotsky to create, with A.R. Luria, his theory of the systemic dynamic localization of higher mental functions and their relationship to cultural conditions. Vygotsky first presented this theory in his report on the Neurological Hospital of Moscow State University on Sept. 9, 1930. “The cerebral bases for mental processes do not lie in some isolated areas of the brain, but in complex systems of the whole brain” (Vygotsky, 1930/1982, p. 128). Very important is the reciprocal interaction between brain maturation and formation of mental functions. For the emergence of a function, a certain degree of maturity of the nervous system is required; but on the other hand, the functioning itself has an active and developing remedial effect, influencing the maturation of structural elements. In this work, Vygotsky also identified 3 steps of these complex systems development: “interpsychological — I order, you perform; then extrapsychological — I order myself; then intrapsychological — two points of the brain, excited from outside, have a tendency to work as part of the same system and become an intracortical point” (Ibid, p. 130). The biggest contribution to this theory came from the assessment of patients in this hospital with Parkinson’s disease.
The study of Parkinson’s disease and mediation theory
“Everybody knows that individuals with Parkinson’s disease climb stairs well but have difficulty walking on the floor. To take a patient to our laboratory we needed to put strips of paper on the floor… An individual with Parkinson’s disease makes a connection between 2 areas of his brain through a peripheral sign.” (Ibid, p. 129). These new formations have a cultural origin, a dynamic psychological structure, and a dynamic brain (body) organization as well. In the late 1920s L.S. Vygotsky and A.R. Luria created a program for compensation of motor subcortical disturbances in Parkinson’s disease (PD) through cortical (visual) mediation of movements. According to Vygotsky and Luria, mediation is a natural process of cognitive development in children, and of psychological compensation for cognitive and physical deterioration in both children and adults. The program they proposed consisted of two main stages: 1) the training stage, when the patient learned to use visual cues, with a gradual decrease in external cueing; and 2) the internalization stage, when the external cues are gradually replaced by their internal images, which become internal means for the patient to control his/her own motor behavior.
In continuing Vygotsky’s and Luria’s work (Sozinova, Glozman, Levin, & Unishenko, 2005) we differentiated 4 steps: 1) the diagnostic phase (determining the degree of walking disturbances and the efficiency of patient rehabilitation); 2) the training phase (walking on strips with the progressive increase of the distance between them); 3) the internalization phase (gradual reduction of the cues, with the instruction to imagine them during walking); and 4) the automation phase (patients walked without strips, singing or reciting a poem, or answering questions while walking).
We also applied different means of mediation for both motor and cognitive rehabilitation of parkinsonian patients. We used visual means (external marks for walking and orientation in space; frames for writing; externalized numbers or signs for counting and attention); semantic means (logical analysis in counting and problem solving; actualization of semantic relations for memorization; actualization of image and word relationships for vocabulary and memorization); and emotional means (computer games for spatial orientation and vocabulary; competitive situations; biological feedback). These complex systems of mediation proved their efficiency both for rehabilitation of parkinsonian patients and remediation of learning disabled children (Glozman, 2011). (Fig. 2).
So, teaching strategies are not only a means to learn culture — to form or to re-mediate mental functions; they are cultural instruments in themselves. “The higher mental function is a social means of behavior, converted within one’s self ” (Vygotsky, 1978).
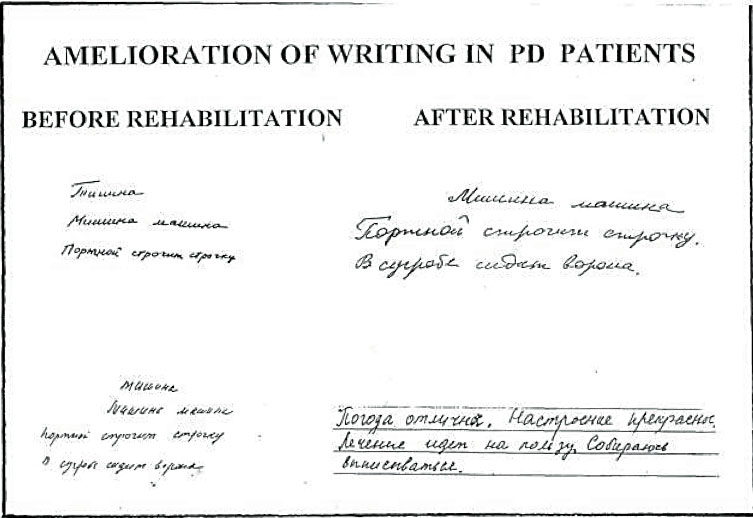
Figure 2. Rehabilitation of micrographia in patients with Parkinson’s disease (PD) by means of visual frames
We also tried to answer the question as to why two patients with the same degree of severity of the disease, similar treatment, and symptomatic regression, have completely different emotional reactions to their situations. To explain this well-known fact, we propose to distinguish between the objective mediating factors, like reeducative techniques and modalities, and subjective mediating factors, like the internal representation of one’s own disease, a factor that determines the quality of life of the patient and his caregiver. This concept of internal representation of one’s own disease was proposed by A.R. Luria’s father, R.A. Luria (1935), to describe “everything the patient feels, the whole complex of his sensations… the patient’s inner world, representing complex combinations of sensations and perceptions, emotions, affections, conflicts and mental trauma” (p. 56). The author described the structure of the internal representation of the disease (IRD), including the sensitive aspect (emotional reaction to one’s own disease), the cognitive aspect (mental representation of one’s own disease), and the voluntary aspect (one’s active attitude toward surmounting the disease). Based on this theory, we proposed three types of internal representation of disease:
1. ANOSOGNOSIC — characterized by low scores for all three aspects of IRD; high cognitive deficiency; a middle score for quality of life of the patient; and a very low score for quality of life of his/her caregiver.
2. HYPOCHONDRIAC — characterized by a high score for sensitive aspect of IRD, middle for the cognitive aspect, and very low for the voluntary one; severe depression; low scores for quality of life for both the patient and his/her caregiver.
3. BALANCED — characterized by high scores for the sensitive and voluntary aspects of IRD, and middle for the cognitive one; high scores for quality of life for both patient and his caregiver.
This classification permits us to define the task required for rehabilitation of subjects with Parkinson’s disease: to form a balanced type of internal representation of the disease as a subjective mediating factor. The proof of the importance of this task is the evidence that a change in internal representation of one’s own disease’s characteristics mediates the reduction of Parkinsonian symptoms with treatment, and a change in the internal representation of one’s own disease precedes symptom change. The role of emotion in regulating the genesis of a psychosomatic syndrome was also proven for patients with essential hypertension (Zinchenko, Pervichko, & Ostroumova, 2013).
In this light, I consider that a patient’s quality of life and satisfaction with treatment should be calculated not so much by the absolute degree of preserved ability (the “quantities” of life, according to Bergsma & Engel, 1998, p. 276), but through the relative preservation, compared with the premorbid level of ability, in the patient’s subjective representation of the disease. Therefore, emotional and social factors, familial and recreational functioning, are closely associated with one’s quality of life. Such an approach, I think, corresponds to Vygotsky’s cultural-historical approach to neuropsychology.
Conclusion
The cooperation of outstanding psychologists L.S. Vygotsky and A.R. Luria on theoretical, experimental, and clinical work was an historic event, a scientific phenomenon, and a turning point in the development of psychological science and applied neuropsychology.
The cultural-historical approach to neuropsychology forces neuropsychologists to re-analyze and re-interpret classic neuropsychological syndromes (Ardila, 2013; Kotik-Friedgut & Ardila, 2014); to develop new assessment procedures more in accordance with the patient’s conditions of life, because it was shown that well-educated and brain-damaged individuals showed neuropsychological performance similar to that of non-brain-damaged but illiterate individuals (Agranovich, 2004; Puente, 2012); and to reconsider the concept of the social brain as a social and cultural determinant and regulator of brain functioning (Glozman & Krukov, 2013). The cultural-historical approach in neuropsychology also permits us to differentiate the biology of health (evaluating MRI and blood tests, IQ, number of symptoms upon DSM-V or MKB-11, and so on), where the patient is a passive object of evaluation, from the psychology of health (the internal representation of one’s own disease, the premorbid value of disturbed activity, self-appraisal, sano-genetic potentials, system of social relations, and more), where the patient is a subject of his/ her own disease.
Vygotsky’s theories and evidence from his clinical work are of fundamental importance for developmental neuropsychology (Glozman, 2011). L.S. Vygotsky and A.R. Luria proved that a defect interferes with a child’s appropriation of his/her culture, but cultural means can help the child overcome the defect. In this way, the cultural-historical approach became, and still is, a methodological basis for remediating education, and clinical neuropsychology becomes more than a scientific or “romantic” activity; it becomes an agent of social action.
Acknowledgments
The study is supported by the Russian Scientific Foundation, project № 14-18- 03253.
References
Agranovich, A. (2004). Cross-cultural differences in neuropsychological performance: A comparison between Russian and American samples. In T.V. Akhutina, J.M. Glozman, L.I. Moskovich, D. Robbins (Eds.) A. R. Luria and Contemporary Psychology: Festschrift Celebrating the Centennial of His Birth. (pp. 181–188). New York: Nova Science. Vygotsky in applied neuropsychology
Ardila, A. (2013). A new neuropsychology for the XXI century. Archives of Clinical Neuropsychology, 28(8), 751–762. doi: 10.1093/arclin/act036
Ardila, A. (2016). The evolutionary concept of “pre-adaptation” applied to cognitive neurosciences. Frontiers in Neuroscience, 10, 103. doi: 10.3389/fnins.2016.00103 Bergsma, J. & Engel, G. (1988). Quality of life: Does measurement help? Health Policy, 10, 267– 279. doi: 10.1016/0168-8510(88)90062-0
Glozman, J. M. (2004). A. N. Leontiev i A. R. Luria (U istokov otechestvennoy neiropsykologii i psykhofiziologii). [A. N. Leontiev and A. R. Luria (Sources of Russian neuropsychology and Psychophysiology] Vestnik Moskovskogo Universiteta. Seriya 14: Psikhologiya [Moscow University Psychology Bulletin], 1, 3–10.
Glozman, J. M. (2011). Remediation of learning disabled children through L. S. Vygotsky’s approach. Psychology in Russia: State of the Art, 4, 268–279. doi: 10.11621/pir.2011.0016
Glozman, J. M., & Krukov, P. (2013). The social brain. Psychology in Russia: State of the Art, 6(3), 68–78. doi: 10.11621/pir.2013.0307
Kotik-Friedgut, B., & Ardila, A. (2014). Cultural historical theory and cultural neuropsychology today. In A. Yasnitsky, A.R. van der Veer, & M. Ferrari (Eds). Handbook of Cultural-Historical Theory. (pp. 378–399). Cambridge: Cambridge University Press. doi: 10.1017/ cbo9781139028097.021
Luria, R. A. (1935). Vnutrennaya kartina bolezni i yatrogennyye zabolevaniya [Internal representation of disease and iatrogenic diseases]. Moscow: Meditsina.
Puente, A. (2012, November). The cultural in cross-cultural neuropsychology. Presentation at the 110th Anniversary of Alexander Luria’s Birthday meeting of the Moscow International Congress, Moscow State University, Moscow, Russia.
Sozinova, E. V., Glozman, J. M., Levin, O. S., & Unishenko, N. A. (2005). Neuropsychological rehabilitation of patients with Parkinson’s disease: efficiency criteria. Psychogeriatria Polska, 2(4), 425–435.
Vygotsky, L. S. (1982). Metodika refleksologicheskogo i psykhologicheskogo issledovania [Method of reflexological and psychological study] In L.S. Vygotsky Collected Papers. (Vol. 1, pp. 43–62). Moscow: Pedagogika. (Original work published 1924)
Vygotsky, L. S. (1925). Principles of social education for deaf and dumb children in Russia. International conference on the education of the deaf. (pp. 227–237). London: William H. Taylor & Sons.
Vygotsky, L. S. (1982). O psykhologicheskih systemakh. [On psychological systems]. In L.S. Vygotsky Collected papers. (Vol. 1, pp. 109–132). Moscow: Pedagogika. (Original work published 1930)
Vygotsky, L. S. (1978). Mind in society. The development of higher psychological processes. Cambridge: Harvard University Press.
Vygotsky, L. S., & Luria, A. R. (1930) Etudy po istorii povedeniya [Studies on the history of behaviour]. Moscow: Gosizdat.
Zinchenko, V. P. (1983) Alexey Nikolaevich Leontiev I razvitie sovremennoy psykhologii. [Alexey Nikolaevich Leontiev and development of contemporary psychology]. In V. V. Davydov, V. P. Zinchenko, A. A. Leontiev, A. V. Petrovsky (Eds.), Selected writings by A. N. Leontiev. (pp. 7–16). Moscow: Pedagogics.
Zinchenko, Yu. P., Pervichko, E. I., & Ostroumova, O. D. (2013). Psychophysiological mechanisms of mental stress reactions in patients with “hypertension at work” and patients with essential hypertension: A comparative analysis. Psychology in Russia: State of the Art, 6(3), 78–94. doi: 10.11621/pir.2013.0308
To cite this article: Glozman J. M. (2016). Vygotsky in applied neuropsychology. Psychology in Russia: State of the Art, 9(4), 73-79.
The journal content is licensed with CC BY-NC “Attribution-NonCommercial” Creative Commons license.







