Validation of Emotional Thermometers as Screening Tools for Mexican Patients Undergoing Breast Biopsies
Sánchez-Jáuregui, T. de J.  Autonomous University of Nuevo Leon, Monterrey, Mexico
Autonomous University of Nuevo Leon, Monterrey, Mexico
Juárez-García, D.M.
Autonomous University of Nuevo Leon, Monterrey, Mexico
Téllez, A.
Autonomous University of Nuevo Leon, Monterrey, Mexico
Abstract
Background. The need to evaluate the emotional changes women experience during the diagnostic stage of breast cancer creates the need for easily applicable short screening tools; thus, evaluations which rely on a single question and visual analogical scales are widely used in hospital environments.
Objective. This study aimed to determine the optimal cut-off points for anxiety, depression, and stress emotional thermometers measured against the Hospital Anxiety and Depression Scale anxiety and depression sub-scales (HADS-A and HADS-D), and the Cohen Perceived Stress Scale-14, respectively; in addition, the study aimed to evaluate the prevalence of these changes in women scheduled for breast biopsies.
Design. The study included 221 women who were scheduled for breast biopsies; their agesranged between28 and80 years old. They were individually evaluated using the Emotional Thermometers, the HADS-A, theHADS-D, and the PSS-14 before undergoingtheir biopsies. Data from 203 participants were analyzed.
Results. The following optimal cut-off points were obtained: 3 for the anxiety emotional thermometer (ET) (sensitivity 0.71, specificity 0.25); 3 for the depression ET (sensitivity 0.87, specificity 0.34); and 4 for the stress ET(sensitivity 0.80, specificity 0.43). According to these cut-off points, 56% of the patients exhibited anxiety, 40% exhibited depression, and 55% exhibited stress.
Conclusion. Using emotional thermometers to screen anxiety, depression, and stress is therefore recommended in the context of breast biopsies.
Received: 24.11.2019
Accepted: 25.12.2019
Themes: Clinical psychology
PDF: http://psychologyinrussia.com/volumes/pdf/2020_2/Psychology_2_2020_96-108_Sanchez.pdf
Pages: 96-108
DOI: 10.11621/pir.2020.0207
Keywords: emotional thermometer; breast biopsy; anxiety; depression; stress
Introduction
Breast cancer is the second most common cancer in the world and the most frequent cancer in women, with approximately two million new cases in 2018 (Ferlay et al., 2019). The early detection of breast cancer is a fundamental strategy for its diagnosis, treatment, and control. In Mexico, the Secretary of Health has placed a permanent screening program in specialized units for women between the ages of 40 and 69 (Uscanga-Sánchez et al., 2014). Of women undergoing a mammography screening, 2-4% are referred for biopsies due to breast abnormalities (Alikhassi et al., 2015; Luiten et al., 2019).
The lesions suspected to be malignant are diagnosed using minimally invasive methods such as stereotactic and ultrasound-guided biopsies, which present the least risks of infection, tissue damage, and invasiveness (Gutwein et al., 2011). Despite this fact, women who undergo these procedures still demonstrate anxiety, physical discomfort, emotional stress, perceived stress, and moderate pain before, during, and after the biopsy procedures. These effects may persist for several weeks after the procedure, even after a woman receives a negative diagnosis for cancer (Bredal et al., 2013; Humphrey et al., 2014; Miller et al., 2013; Miller et al., 2014; Witek-Janusek et al., 2007).
The risk of a possible diagnosis, the invasiveness of the procedure, anxiety as a personality trait, chronic stress, and the level of coping skills are some of the most important psychosocial variables associated with anxiety before and after a breast biopsy (Raineri et al., 2019).
It has been recommended that all oncological patients undergo psychological evaluation as part of their standard treatment. Detection and treatment of psychological problems has been justified by the fact that patients with higher levels of psychological discomfort require more medical services, exhibit low adaptation to disease, are less likely to adhere to treatment plans, and have a higher degree of difficulty in making decisions. They also show more dissatisfaction with the medical care received, and a lowering of quality of life; such psychological discomforts are also associated with lower longevity (Jadoon, et al., 2010; Vázquez et al., 2013).
Furthermore, it has been found that stress and anxiety can influence post-surgery recovery time, the use of analgesics, and the length of hospital stay (Jiménez-Jiménez et al., 2013; Mavros et al., 2011; Montgomery et al., 2007; Tefikow et al., 2013).
Previous studies have shown that anxiety has negative consequences before, during, and after biopsy procedures. As far as we know, there have been no studies in Mexico that report on anxiety levels, depression, or stress in patients during biopsy programs; nor are there studies that validate an analogous visual scale to measure these variables.
The use of short screening tools such as visual analogue scales (VAS), which are easily implemented in hospital environments, is recommended for identifying patients who initially display symptoms of anxiety and/or depression; these patients can then be referred for subsequent and more thorough examinations so that they may receive adequate psychological care (Almanza-Muñoz et al., 2009; Boyes et al., 2013). Some researchers have found a substantial correlation between the levels of stress, anxiety, and depression measured by VAS, and those measured by the Cohen Perceived Stress Scales (PSS) and the Hospital Anxiety and Depression Scale (HADS) in both medical personnel (Lesage et al., 2012) and cancer patients (Grassi et al., 2009; Lambert et al., 2014).
Roth et al. (1998) developed a distress thermometer for patients with prostate cancer. Subsequently, Mitchell et al. (2010) validated an emotional thermometer (ET) that incorporates analogue visual scales for depression and anxiety in cancer patients before their first chemotherapy treatment. However, as suggested by Ma et al. (2014), additional studies are needed to determine the accuracy and optimal cutoff point for ETs in different populations, as well as under different medical conditions, since the use of short scales as a screening tool for emotional changes during the diagnostic stage, particularly during breast biopsy, has not been widely studied.
The National Comprehensive Cancer Network (NCCN, 2018) recommends using the distress thermometer developed by Roth et al. in 1998. However, in some countries, including Spanish-speaking regions, the translation of the term “distress” is problematic because of a lack of a precise conceptual and operational definition of the term; thus it results in the use of different assessment tools. Additionally, different terms are used as synonyms for distress: i.e.,stress, anxiety, anger, tension, confusion, depression, intrusion, being sad, and feeling bad (Donovan et al., 2014; Gil et al., 2005; Montgomery & McCrone, 2010; Muszbek et al., 2006; Potter, 2007; Romito et al., 2013). This imprecision results in a risk of measuring different dimensions, whereas terms such as depression, anxiety, and stress are easily translated and understood, leading us to recommend measuring each of these variables separately.
Most studies ofemotional thermometershave been carried out in Europe; thus, data is needed from Latin America and at different stages of cancer development (Harju et al., 2019).
The main objectives of this study were to determine the optimal cut-off points for the anxiety ET, depression ET, and stress ET measured against the Hospital Anxiety and Depression Scale for anxiety (HADS-A), the HADS for depression (HADS-D), and the Perceived Stress Scale (PSS-14), respectively, in women scheduled for breast biopsies, and to evaluate the prevalence of anxiety, depression, and stress in this population.
Methods
Participants
A non-probabilistic sample was used. A total of 221 women scheduled for ultrasound or a stereotactic-guided breast biopsies was invited to participate in the study. Of these, three refused to participate and nine did not complete the survey; six women did not meet the inclusion criteria, which included: 1) falling within the range of 28 to 80 years of age; 2) having had no previous breast biopsy; 3) being able to read and write in Spanish; and 4) having had no previous diagnosis of cancer, psychiatric disorder, or mental deficiency. In the end, the data from 203 participants were analyzed (Figure 1).
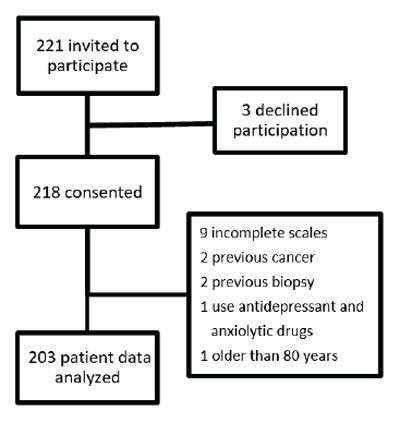
Figure 1. Flow diagram
The study was approved by the Bioethics Committee of the Bernardo Sepúlveda Hospital of the Secretary of Health of Nuevo León (protocol #14/597), where it was conducted. The samples were collected between January 2015 and December 2016.
Procedure
All patients who required biopsies due to abnormalities in their mammograms had been referred to the psychology department for evaluation by the surgeon of the breast disease clinic and the department of radiology. After signing the informed consent form, each individual patient underwent a semi-structured interview for the collection of sociodemographic data; then they were individually evaluated using the Emotional Thermometers, the HADS-A, HADS-D, and the PSS-14 before undergoing their biopsy. Each patient was briefly informed of what the emotional thermometer consists of and the variables being studied: anxiety, depression, and stress. The application of the evaluation instruments was conducted in the psychology department of the hospital by trained psychologists.
Questionnaires
A sociodemographic questionnaire was used for obtaining information regarding each woman’s age, level of education, marital status, number of children, and socioeconomic status. To evaluate anxiety, depression, and stress, the following tools were used.
The Hospital Anxiety and Depression Scale (HADS) was developed by Zigmond and Snaith in 1982 and comprises a total of 14 questions: seven for measuring anxiety (HADS-A) and seven for measuring depression (HADS-D). The Spanish version of the scale developed by Tejero, Guimerá, and Farré (1986) which has a Cronbach’s alpha coefficient of .80, was used in the present study. The HADS evaluates the psychological aspects of anxiety and depression, but does not consider symptoms such as insomnia, fatigue, and appetite loss. In each subscale, readings above the cut-off point of 8 indicate changes on the clinical level.
The Perceived Stress Scale (PSS-14) of Cohen, Kamarck, and Mermelstein (1983) contains 14 questions and evaluates the degree to which life situations are perceived as stressful by an individual. The questions are classified on a 5-point Likert scale (0 = never, 1 = almost never, 2 = sometimes, 3 = often, and 4 = very often). A larger score indicates a greater level of stress. The present study used the scale’s Mexican version developed by González and Landero (2007). González-Ramírez, Rodríguez-Ayán, and Hernández (2013) proposed that a standard deviation above the mean can be used as an indicator of clinical stress.
The Emotional Thermometer (ET), developed by Mitchell et al. (2010), is a combination of five visual analogical scales that measure stress, anxiety, depression, anger, and the need for help. These scales contain 11 degrees from 0 to 10, with 0 representing the absence of the emotion, and 10 the maximum level of the perceived emotion. The recommended cut-off point for all the scales is 3 vs 4, with a sensibility of 92% and specificity of 61% for the anxiety thermometer, and a sensibility of 60% and specificity of 78% for the depression thermometer, as compared with the HADS subscales. For the present study, only the anxiety and depression thermometers were used, and a thermometer for measuring stress was added.
Statistical analysis
The statistical analyses were performed using Windows program SPSS 21. For validating the optimal cut-off point of the anxiety ET,the point system of the HADS-A subscale was used (cut-off 7 vs 8); for the depression ET, the point system of the HADS-D was used (cut-off 7 vs 8), as recommended by Mitchell et al., (2010); and for the stress ET, the point system obtained in the PSS-14 was used, as recommended by González-Ramírez, et al. (2013). They propose that the average of the group, plus one standard deviation, should be considered as indicative of stress on a clinical level (cut-off 27 vs 28).
Using a 2 × 2 table, the Positive Predictive Values (PPV) [(true positive/total positive)] and Negative Predictive Value (NPV) [(true negative/total negative)] were obtained. A Receiver Operating Curve (ROC) was generated through which the Area Under the Curve (AUC), sensibility, and specificity were obtained. A Spearman correlation was performed to determine the effect size (small =.10, medium =.30, and large ≥ .50) between the variables (Téllez et al., 2015). Finally, based on the cut-off points, the frequencies and percentages of women who exhibited anxiety, stress, and depression were obtained.
Results
Socio-demographic data
Of the 221 patients who consented to participate, 203 were evaluated using the various tools. The average age of the participants was 48 years (SD = 10.9), 64.8% lived in a conjugal relationship, and 28.6% were employed. The average number of years of education was 8.4 (SD=3.7), and the average monthly income was 193 U.S. Dollars (SD = 214 USD).
Properties of the ETs as diagnostic tests
Table 1presents the cut-off points that are considered most adequate according to the ROC. For the cut-off point of 3 on the anxiety ET, an AUC of .789 was obtained [95% confidence interval (CI) = .726, .852; p =.000]; for the cut-off point of 3 on the depressionET, an AUC of .855 was obtained [95% CI = .784−.925; p =.000]; and for the cut-off point of 4 on the stressET, an AUC of .734 was obtained [95% CI= .629–.839; p = .001].
|
Table 1 Psychometric properties of the ETs |
|||||
|
|
Sensitivity |
Specificity |
PPV |
NPV |
Accuracy |
|
ET Anxiety Cut-off 3 |
0.71 |
0.25 |
0.75 |
0.70 |
.789 |
|
ETDepression Cut-off 3 |
0.87 |
0.34 |
0.25 |
0.97 |
.855 |
|
ET Stress Cut-off 4 |
0.80 |
0.43 |
0.15 |
0.96 |
.734 |
ET= Emotional Thermometer, PPV=Positive Predictive Value, VPN=Negative Predictive Value
The correlation analysis between the scales shows a positive correlation with a large and statistically significant effect size between the HADS-A subscale and the ETanxiety scale (rs = .633, p = .01), as well as between the HADS depression sub-scale and the ETdepression scale (rs = .566, p = .01). A positive correlation with a medium-large effect size was also found between the PSS-14 and the ETstress scales (rs =. 403, p = .01).
Prevalence of anxiety, depression, and stress according to the cut-off points obtained
The average score on the anxiety ET was 3.7 (SD = 3.2) and for the HADS-A was 7.7 (SD = 4.2); for the depression ETthe average score was 3.2 (SD = 3.3) and 3.7 on the HADS-D (SD = 3.1). The average obtained for the stressET was 4.0 (SD = 3.0), and on the PSS-14 the average was 21.3 (SD = 7.5).
According to the cut-off points used in the ETs, 56 % of the patients exhibited anxiety, 40% exhibited depression, and 55% exhibited symptoms of stress (Figure 2).
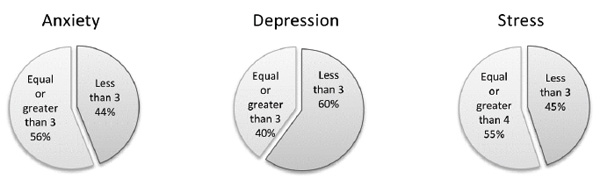
Figure 2. Prevalence of anxiety, depression, and stress
Discussion
The primary objective of this study was to determine the optimal cut-off points for the anxiety and depression thermometers as compared to the HADS scale for evaluating anxiety and depression, and the same for the stress thermometer measured against the PSS-14. Although the thermometers were applied to women who had not yet been diagnosed with cancer, a cut-off point of 3 for anxiety and depression, and 4 for stress, coheres with the results ofMitchell et al. (2010), who suggested a cut-off point of 3 vs 4 for all the thermometers used with cancer patients; and with those of Beck et al. (2016), who found a cut-off point of 4 for anxiety and 3 for depression in patients with different types of cancer. Shahvaroughi et al. (2019) have also established a cut-off point of 3 for the Persian version of the anxiety and depression thermometers in Iranian patients with advanced cancer.
Some other studies have found different cut-off points than we did in this study. For instance, Teixeira et al. (2020) found a cut-off point of 5 vs 6 for anxiety, and 4 vs 5 for depression in a validation of emotional thermometers in Portuguese patients receiving treatment for different types of cancer. Civilotti et al. (2020) applied the distress thermometer against HADS in patients with a recent diagnosis of breast cancer, recommending a cut-off point of 4 for anxiety, depression and distress. A systematic review by Harju et al. (2019) found that most authors suggest a cut-off point to be equal or higher than 4 for anxiety and depression thermometers. Probablythe differences in the results of those authors and our study is due to the different instrumentsused to validate the thermometers.
The original study involving the emotional thermometers developed by Mitchell et al. (2010) found an average of 4.78 for anxietyleveland 2.34 for depression, while our study found average levels of 3.7 for anxiety, 3.2 for depression, and 4 for stress. These scores are higher than those reported by Hinz et al. (2019) in the general German population; they found an average of 1.3 for anxiety level and 1.6 for depression. The slight differences in the results obtained in both studies may be explained by differences between the medical conditions and demographics of the patients.
The averages of 7.7 for anxiety measured using the HADS-A, 3.7 for depression measured using the HADS-D, and 21.3 for stress using the PSS-14 corroborate the results obtained by other authors for anxiety and depression before biopsies (Lampic et al., 2001; Dey et al., 2002; Kamath et al., 2012). On the other hand, Gibbons et al. (2016) obtained an average of 23.4 for stress at the time of diagnosis.
In the present study, the anxiety, depression, and stress ETsdisplayed adequate levels of sensibility at >.70, demonstrating that they have a greater ability to detect patients undergoing these changes; however, they also displayed low levels of specificity at <.50, which may hinder their ability to screen those without such changes, thus potentially increasing the probability of false positives. However, in the present study scenario, it is preferable to detect the majority of patients who do exhibit emotional changes.
As for the predictive value, it was observed that the depression and stress ETs display a high NPV, thus reflecting a low prevalence of these symptoms in the studied population (Colimon, 1990); however, a high NPV minimizes the false negatives, and an optimal cut-off point for screening based on a specific population requires a minimum number of false negatives (Bidstrup et al., 2012). The predictive values for both positives and negatives for the anxiety ET yield a result of 70%, reflecting a prevalence of approximately 50%. This is in agreement with the prevalence results obtained in this study based on the cut-off points selected.
However, the AUC provides a means to discriminate between those people who experience the variable of interest vs those who do not. An AUC value between 0.7 and 0.8 is considered in line with acceptable discrimination (Hosmer & Lemeshow, 2000), in addition to being an indicator of diagnostic exactness (Schubart et al., 2015). The three thermometers we measured achieved adequate AUC values, which, in addition to the results obtained from the correlation between the ETs, the HADSs, and the PSS-14, indicates that the ETs may be used to detect patients who require a more thorough evaluation for anxiety, depression, and stress. These results for sensibility, specificity, and AUC are similar to those reported by Mitchell et al. (2010) for selected cut-off points in patients with cancer.
In our sample, 56% of the patients exhibited anxiety, 40% exhibited depression, and 55% exhibited stress symptoms; that is, approximately half of the patients presented some type of emotional change related to the biopsy procedure. In a study of the diagnostic period involving mammograms and biopsies, Lampic et al. (2001) found that of 509 patients, 46% exhibited anxiety and 11% exhibited depression. In a recent study, Moseholm et al. (2016) found that 34% of a sample of 666 patients with all types of cancer, exhibited anxiety, and 24% exhibited depression before the diagnosis. Similar data was found by Civilotti et al. (2020) in Italian women with newly diagnosed cancers; 52.1% of the women affected by breast cancer presented anxiety symptoms, whereas 33% presented depressive symptoms. Regarding stress, Turkoglu and Mutlu (2016) found that 33% of patients exhibited stress before undergoing any type of biopsy.
Research into psychological disorders and tools used during the diagnostic process could help identify women who are at risk for chronic psychological problems and social isolation during their cancer treatments. This in turn could help identify risk and protective factors for these women and help to develop specific intervention techniques for them (Kamath et al., 2012). For example, Perlman et al. (2016) suggest that strategies for improving the mood of women who are facing breast biopsies could greatly benefit them. Téllez et al. (2016) and Sánchez-Jáuregui et al. (2018) used an intervention with hypnosis and music, and found a decrease in anxiety, stress, and pain, as well as an increase in optimism and well-being both before and after the biopsy. Furthermore, to improve the biopsy experience, Soo et al. (2019), recommend giving information about the procedure before the biopsy, providing a comfortable and private waiting room space, and using local anesthesia, anxiolytics, or psychotherapeutic interventions such as hypnosis, relaxing music, and guided meditation.
To the best of our knowledge, ours is the first study reporting the adequate adaptation of ETs for women scheduled for breast tissue biopsies. The thermometers are a useful and reliable tool to screen emotional changes in a hospital environment, allowing medical personnel to identify patients who display results above the cut-off point, and to channel them for more thorough psychological evaluation.
Finally, although the importance of evaluating psychological changes during the medical procedures and the usefulness of short tests such as ETs has already been demonstrated, less than 15% of medical personnel use screening tools in clinical practice (Mitchell et al., 2008). Therefore, we strongly recommend using this tool as a regular part of the medical routine in the context of the diagnosis of breast cancer.
Conclusion
The evaluation of emotional changes during the biopsy procedure for suspected breast cancer is important. The anxiety, depression, and stress ETs are precise screening tools when used with the cut-off points suggested in the present study. In addition, they are low-cost and easily applicable in a hospital context.
Limitations
Our study has some limitations, such as the fact that the validation of the emotional thermometers was done by comparing them with the HADS subscales, in which low scores of anxiety and depression were obtained. Thus, in future studies it would be advisable to use other standardized diagnostic scales, such as the Structured Clinical Interview for DSM–IV to confirm the results. It is also important to consider that the population we studied has a low degree of education and income, so the results cannot be generalized to populations with different characteristics.
Acknowledgements
This research was supported by the Mexican Avon Breast Cancer Crusade, 2016 (Project No. 66).
References
Alikhassi, A., Ahmadinejad, N., Sedighi, N., & Najafi, M. (2015). Stereotactic Breast Core Needle Biopsy in a Tertiary Breast Center of the Tehran University of Medical Sciences. Archives of Breast Cancer, 2, 21-26. https://doi.org/10.19187/abc.20152121-26
Almanza-Muñoz, J.J., Rosario-Juárez, I., Silva-Ortiz, J., & de la Huerta-Sánchez, R. (2009). Distrés psicosocial y trastornos mentales en una muestra de pacientes mexicanos con cáncer. [Psychosocial stress and mental disorders in a sample of Mexican patients with cancer]. Revista de Sanidad Militar, 63, 148-155.https://www.medigraphic.com/pdfs/sanmil/sm-2009/sm094b.pdf
Beck, K.R., Tan, S.M., Lum, S.S., Lim, L.E., & Krishna, L.K. (2016). Validation of the emotion thermometers and hospital anxiety and depression scales in Singapore: screening cancer patients for distress, anxiety and depression. Asia Pacific Journal of Clinical Oncology. 12, e241–e249. https://doi.org/10.1111/ajco.12180
Bidstrup, P.E., Mertz, B.G., Dalton, S.O., Deltour, I., Kroman, N., Kehlet, H., … Johansen, C. (2012). Accuracy of the Danish version of the “distress thermometer.” Psycho-Oncology, 21, 436-443. https://doi.org/10.1002/pon.1917
Boyes, A., D’Este, C., Carey, M., Lecathelinais, C., & Girgis, A. (2013). How does the Distress Thermometer compare to the Hospital Anxiety and Depression Scale for detecting possible cases of psychological morbidity among cancer survivors? Supportive Care in Cancer, 21, 119-127. https://doi.org/10.1007/s00520-012-1499-3
Bredal, I.S., Kåresen, R., Skaane, P., Engelstad, K.S., & Ekeberg, Ø. (2013). Recall mammography and psychological distress. European Journal of Cancer,49,805-811. https://doi.org/10.1016/j.ejca.2012.09.001
Civilotti, C., Maran, D.A., Santagata, F., Varetto, A., & Stanizzo, M.R. (2020). The use of the Distress Thermometer and the Hospital Anxiety and Depression Scale for screening of anxiety and depression in Italian women newly diagnosed with breast cancer. Supportive Care in Cancer, 1-8. https://doi.org/10.1007/s00520-020-05343-x
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385-396.https://doi.org/10.2307/2136404
Colimon, K.M. (1990). Fundamentos de epidemiología. Ediciones Díaz de Santos.
Dey, P., Dixon, J.M., Bundred, N., Gibbs, A., Hopwood, P., Baildam, A.… Woodman, C. (2002). Costs and benefits of a one stop clinic compared with a dedicated breast clinic: a randomised controlled trial. Commentary: one stop clinics should not be abandoned. British Medical Journal, 324, 507-510. https://doi.org/10.1136/bmj.324.7336.507
Donovan, K.A., Grassi, L., McGinty, H.L., & Jacobsen, P.B. (2014). Validation of the distress thermometer worldwide: state of the science. Psycho-Oncology, 23, 241-250. https://doi.org/10.1002/pon.3430
Ferlay, J., Colombet, M., Soerjomataram, I., Mathers, C., Parkin, D.M., Piñeros, M. … Bray, F. (2019). Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. International Journal of Cancer, 144(8), 1941-1953. https://doi.org/10.1002/ijc.31937
Gibbons, A., Groarke, A., Curtis, R., & Groarke, J. (2016). The effect of mode of detection of breast cancer on stress and distress. Psycho-Oncology, 26(6), 787-792. https://doi.org/10.1002/pon.4227
Gil, F., Grassi, L., Travado, L., Tomamichel, M., Gonzalez, J.R., & SEPOS Group. (2005). Use of distress and depression thermometers to measure psychosocial morbidity among southern European cancer patients. Supportive Care in Cancer, 13, 600-606. https://doi.org/10.1007/s00520-005-0780-0
González, M.T., & Landero, R. (2007). Factor structure of the perceived Stress Scale (PPS) in a Sample from Mexico. The Spanish Journal of Psychology, 10, 201- 208.https://doi.org/10.1017/S1138741600006466
González-Ramírez, M.T., Rodríguez-Ayán, M.N., & Hernández, R.L. (2013). The Perceived Stress Scale (PSS): Normative data and factor structure for a large-scale sample in Mexico. The Spanish Journal of Psychology, 16, E47, 1-9. https://doi.org/10.1017/sjp.2013.35
Grassi, L., Sabato, S., Rossi, E., Marmai, L., & Biancosino, B. (2009). Affective syndromes and their screening in cancer patients with early and stable disease: Italian ICD-10 data and performance of the Distress Thermometer from the Southern European Psycho-Oncology Study (SEPOS). Journal of Affective Disorders, 114, 193-199. https://doi.org/10.1016/j.jad.2008.07.016
Gutwein, L.G., Ang, D.N., Liu, H., Marshall, J.K., Hochwald, S.N., Copeland, E. M., & Grobmyer, S.R. (2011). Utilization of minimally invasive breast biopsy for the evaluation of suspicious breast lesions. The American Journal of Surgery, 202, 127-132. https://doi.org/10.1016/J.AMJSURG.2010.09.005
Harju, E., Michel, G., & Roser, K. (2019). A systematic review on the use of the emotion thermometer in individuals diagnosed with cancer. Psycho-oncology, 28(9), 1803-1818. https://doi.org/10.1002/pon.5172
Hinz, A., Mitchell, A. J., Dégi, C.L., & Mehnert-Theuerkauf, A. (2019). Normative values for the distress thermometer (DT) and the emotion thermometers (ET), derived from a German general population sample. Quality of Life Research, 28(1), 277-282.https://doi.org/10.1007/s11136-018-2014-1
Hosmer, D.W., & Lemeshow, S. (2000). Interpretation of the Fitted Logistic Regression Model, in Applied Logistic Regression, Second Edition, NJ, USA: John Wiley & Sons, Inc., Hoboken. https://doi.org/10.1002/0471722146.ch3
Humphrey, K.L., Lee, J.M., Donelan, K., Kong, C.Y., Williams, O., Itauma, O., … Swan, J.S. (2014). Percutaneous Breast Biopsy: Effect on Short-term Quality of Life. Radiology, 270, 362-368. https://doi.org/10.1148/radiol.13130865
Jadoon, N.A., Munir, W., Shahzad, M.A., & Choudhry, Z.S. (2010). Assessment of depression and anxiety in adult cancer outpatients: a cross-sectional study. BMCancer, 10(1), 594. https://doi.org/10.2147/COAYA.S29735
Jiménez-Jiménez, M., García-Escalona, A., Martín-López, A., De Vera-Vera, R., & De Haro, J. (2013). Intraoperative stress and anxiety reduction with music therapy: A controlled randomized clinical trial of efficacy and safety. Journal of Vascular Nursing, 31(3), 101-106. https://doi.org/10.1016/j.jvn.2012.10.002
Kamath, J., Cruess, D.G., Claffey, K., Wilson, L., Phoenix, N., & Tannenbaum, S. (2012). Symptom distress associated with biopsy in women with suspect breast lesions. International Scholarly Research Network Oncology,2012, 1-9. https://doi.org/10.5402/2012/898327
Lambert, S.D., Pallant, J.F., Clover, K., Britton, B., King, M.T., & Carter, G. (2014). Using Rasch analysis to examine the distress thermometer’s cut-off scores among a mixed group of patients with cancer. Quality of Life Research, 23, 2257-2265. https://doi.org/10.1007/s11136-014-0673-0
Lampic, C., Thurfjell, E., Bergh, J., & Sjödén, P.O. (2001). Short-and long-term anxiety and depression in women recalled after breast cancer screening. European Journal of Cancer, 37, 463-469. https://doi.org/10.1016/S0959-8049(00)00426-3
Lesage, F.X., Berjot, S., & Deschamps, F. (2012). Clinical stress assessment using a visual analogue scale.Occupational medicine, 62, 600-605. https://doi.org/10.1093/occmed/kqs140
Luiten, J.D., Korte, B., Voogd, A.C., Vreuls, W., Luiten, E.J., Strobbe, L.J., … Duijm, L.E. (2019). Trends in frequency and outcome of high‐risk breast lesions at core needle biopsy in women recalled at biennial screening mammography, a multi-institutional study. International Journal of Cancer, 145(10), 2720-2727. https://doi.org/10.1002/ijc.32353
Ma, X., Zhang, J., Zhong, W., Shu, C., Wang, F., Wen, J., … Liu, L. (2014). The diagnostic role of a short screening tool—the distress thermometer: a meta-analysis. Supportive Care in Cancer, 2, 1741-1755. https://doi.org/10.1007/s00520-014-2143-1
Mavros, M.N., Athanasiou, S., Gkegkes, I.D., Polyzos, K.A., Peppas, G., & Falagas, M.E. (2011). Do psychological variables affect early surgical recovery? PLoS One, 6(5), e20306. http://dx.doi.org/10.1371/journal.pone.0020306.
Miller, L.S., Shelby, R.A., Balmadrid, M.H., Yoon, S., Baker, J.A., Wildermann, L., & Soo, M.S. (2013). Patient anxiety before and immediately after imaging-guided breast biopsy procedures: impact of radiologist-patient communication. Journal of the American College of Radiology, 10, 423-431. https://doi.org/10.1016/j.jacr.2012.11.005
Miller, S.J., Sohl, S.J., Schnur, J.B., Margolies, L., Bolno, J., Szabo, J., … Montgomery, G.H. (2014). Pre-Biopsy Psychological Factors Predict Patient Biopsy Experience. International Journal of Behavioral Medicine, 21, 144-148. https://doi.org/10.1007/s12529-012-9274-x
Mitchell, A.J., Baker‐Glenn, E.A., Granger, L., & Symonds, P. (2010). Can the Distress Thermometer be improved by additional mood domains? Part I. Initial validation of the Emotion Thermometers tool. Psycho-Oncology, 19, 125-133.https://doi.org/10.1002/pon.1523
Mitchell, A.J., Kaar, S., Coggan, C., & Herdman, J. (2008). Acceptability of common screening methods used to detect distress and related mood disorders—preferences of cancer specialists and non‐specialists. Psycho-Oncology, 17, 226-236. https://doi.org/10.1002/pon.1228
Montgomery, G.H., Bovbjerg, D.H., Schnur, J.B., David, D., Goldfarb, A., Weltz, C.R., … Silverstein, J.H. (2007). A randomized clinical trial of a brief hypnosis intervention to control side effects in breast surgery patients. Journal of the National Cancer Institute, 99(17), 1304-1312. https://doi.org/10.1093/jnci/djm106
Montgomery, M., & McCrone, S.H. (2010). Psychological distress associated with the diagnostic phase for suspected breast cancer: systematic review. Journal of Advanced Nursing, 66, 2372-2390. https://doi.org/10.1111/j.1365-2648.2010.05439.x
Moseholm, E., Rydahl-Hansen, S., Overgaard, D., Wengel, H.S., Frederiksen, R., Brandt, M., & Lindhardt, B.Ø. (2016). Health-related quality of life, anxiety and depression in the diagnostic phase of suspected cancer, and the influence of diagnosis. Health and Quality of Life Outcomes, 14, 1-12.https://doi.org/10.1186/s12955-016-0484-9
Muszbek, K., Szekely, A., Balogh, É.M., Molnár, M., Rohánszky, M., Ruzsa, Á.,… Vadász, P. (2006). Validation of the Hungarian translation of hospital anxiety and depression scale. Quality of Life Research, 15, 761-766. https://doi.org/10.1007/s11136-005-3627-8
National Comprehensive Cancer Network (2018). NCCN Guidelines for Patients: Distress, Version 1.2017. https://www.nccn.org/patients/guidelines/distress/files/assets/basic-html/page-1.html
Perlman, K.L., Shelby, RA., Wren, A.A., Kelleher, S.A., Dorfman, C.S., O’Connor, E., … Soo, M.S. (2016). Positive and negative mood following imaging-guided core needle breast biopsy and receipt of biopsy results. Psychology, Health & Medicine,1-14. https://doi.org/10.1080/13548506.2016.1271438
Potter, P.J. (2007). Breast Biopsy and Distress Feasibility of Testing a Reiki Intervention. Journal of Holistic Nursing, 25, 238-248. https://doi.org/10.1177/0898010107301618
Raineri, A.M., Pelagotti, S., & Grotto, R.L. (2019). Sveva: development and evaluation of a supportive care model to reduce breast biopsy pre-operative anxiety: a randomized case-control study. Mediterranean Journal of Clinical Psychology,7(3). https://doi.org/10.6092/2282-1619/2019.7.2169
Romito, F., Lagattolla, F., Costanzo, C., Giotta, F., & Mattioli, V. (2013). Music therapy and emotional expression during chemotherapy. How do breast cancer patients feel? European Journal of Integrative Medicine, 5, 438-442. https://doi.org/10.1016/j.eujim.2013.04.001
Roth, A.J., Kornblith, A.B., Batel-Copel, L., Peabody, E., Scher, H.I., & Holland, J. C. (1998). Rapid screening for psychologic distress in men with prostate carcinoma. Cancer, 82, 1904-1908. https://doi.org/10.1002/(SICI)1097-0142(19980515)82:10<1904::AID-CNCR13>3.0.CO;2-X
Sánchez-Jáuregui, T., Téllez, A., Juárez-García, D., García, C.H., & García, F.E. (2018). Clinical hypnosis and music in breast biopsy: a randomized clinical trial. American Journal of Clinical Hypnosis, 61(3), 244-257. https://doi.org/10.1080/00029157.2018.1489776
Shahvaroughi Farahani N., Bastami, M., Alemrajabi, M., Alasty, H., & Rajabi, M. (2019). Validity and Reliability of the Persian Version of Emotion Thermometers in Iranian Advanced Cancer Patients. International Journal of Cancer Management, 12(7). http://doi.org/10.5812/ijcm.90504
Schubart, J.R., Mitchell, A.J., Dietrich, L., & Gusani, N.J. (2015). Accuracy of the Emotion Thermometers (ET) screening tool in patients undergoing surgery for upper gastrointestinal malignancies. Journal of Psychosocial Oncology, 33(1), 1-14. https://doi.org/10.1080/07347332.2014.977415
Soo, M.S., Shelby, R.A., & Johnson, K.S. (2019). Optimizing the patient experience during breast biopsy. Journal of Breast Imaging, 1(2), 131-138.https://doi.org/10.1093/jbi/wbz001
Tefikow, S., Barth, J., Maichrowitz, S., Beelmann, A., Strauss, B., & Rosendahl, J. (2013). Efficacy of hypnosis in adults undergoing surgery or medical procedures: A meta-analysis of randomized controlled trials. Clinical Psychology Review, 33(5), 623-636. https://doi.org/10.1016/j.cpr.2013.03.005
Tejero, A., Guimerá, E.M., & Farré, J.M. (1986). Uso clínico del HAD (Hospital Anxiety and Depression Scale) en población psiquiátrica: un estudio de su sensibilidad, fiabilidad y validez. Revista Psiquiátrica de la Facultad de Medicina de Barcelona, 13, 233-238.
Téllez, A., García, C.H., & Corral-Verdugo, V. (2015). Effect size, confidence intervals, and statistical power in psychological research. Psychology in Russia: State of the Art, 8, 1-20. https://doi.org/10.11621/pir.2015.0303
Teixeira, R.J., Machado, J.C., Faria, S., Remondes-Costa, S., Brandão, T., Branco, M., … Pereira, M.G. (2020). Brief emotional screening in oncology: Specificity and sensitivity of the emotion thermometers in the Portuguese cancer population. Palliative & Supportive Care, 18, 39-46. https://doi.org/10.1017/S1478951519000208
Téllez, A., Sánchez-Jáuregui, T., Juárez-García, D.M., & García-Solís, M. (2016). Breast Biopsy: The Effects of Hypnosis and Music. International Journal of Clinical and Experimental Hypnosis, 64, 456-469. https://doi.org/10.1080/00207144.2016.1209034
Turkoglu, O., & Mutlu, H.H. (2016). Evaluation of Stress Scores throughout Radiological Biopsies. Iranian Journal of Radiology, 13, e37978. https://doi.org/10.5812/iranjradiol.37978
Uscanga-Sánchez, S., Torres-Mejía, G., Ángeles-Llerena, A., Domínguez-Malpica, R., & Lazcano-Ponce, E. (2014). Indicadores del proceso de tamizaje de cáncer de mama en México: un estudio de caso. Salud Pública de México, 56,528-537. https://www.scielosp.org/article/spm/2014.v56n5/528-537/
Vázquez, O.G., Martínez, M.M., Ugalde, S.C., Castillo, E.R., Vázquez, M.C.M., & Aguilar, S.A. (2013). Tamizaje de aspectos psico-oncológicos: validación de una lista de chequeo. Psicooncología, 10(2-3), 407-415. https://doi.org/10.5209/rev_PSIC.2013.v10.n2-3.43458
Witek-Janusek, L., Gabram, S., & Mathews, H.L. (2007). Psychologic stress, reduced NK cell activity, and cytokine dysregulation in women experiencing diagnostic breast biopsy. Psychoneuroendocrinology, 32, 22-35. https://doi.org/10.1016/j.psyneuen.2006.09.011
Zigmond, A.S., & Snaith, R.P. (1982). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67, 361-370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x
To cite this article: Sánchez-Jáuregui, T.J., Juárez-García, D.M., Téllez, A. (2020). Validation of Emotional Thermometers as Screening Tools for Mexican Patients Undergoing Breast Biopsies. Psychology in Russia: State of the Art, 13(2), 96-108.
The journal content is licensed with CC BY-NC “Attribution-NonCommercial” Creative Commons license.







