Developmental Change in Full- and Preterm Infants between the Ages of Three and Nine Months in Institutions with Different Caregiving Environments
Abstract
Background. Studies of children raised in institutions have shown that they are at substantial risk in various domains of functioning, but these studies have not examined the children’s developmental change at the very early period of institutionalization.
Objective. The main aim of this study was to examine the behavioral development of institutionalized infants between three and nine months of life as a function of their birth circumstances and the nature of their institutional care.
Design. General behavioral development was studied in 58 (34 males) infants from two St. Petersburg (Russian Federation) institutions (Baby Homes, BH). The infants were divided into four groups according to 1) their gestational age—full-term children (FCh) of 37-41 weeks gestational age, or preterm children (PCh) of 30-36 weeks gestational age; and 2) the type of institutional care environment—either the typical socio-emotionally depriving, non-intervention Baby Home (NoI BH), or an institution that had undergone a program of training plus structural changes intervention (T+SC BH). All the children were assessed at approximately three and nine months of age with the Battelle Development Inventory (BDI; LINK Associates, 1988).
Results. Both the FCh and PCh children from the NoI BH displayed significant declines in their BDI Total scores between three and nine months, whereas only the FCh children in T+SC BH improved over this period of time. In general, the FCh group had higher mean BDI Total developmental quotients (DQs) than the PCh group, and children from the T+SCh BH displayed higher scores than children from the NoI institution.
Conclusion. Thus, the current study showed that the impact of spending their early months in an institution on infants’ development depends on the gestational age of children and the type of institutional care environment.
Received: 22.02.2018
Accepted: 31.07.2018
Themes: Developmental psychology
PDF: http://psychologyinrussia.com/volumes/pdf/2018_3/psych_3_2018_11_Muhamedrahimov.pdf
Pages: 152-167
DOI: 10.11621/pir.2018.0311
Keywords: institutions, full-term (FCh) and preterm (PCh) infants, time, intervention, development
Introduction
The literature on the developmental and behavioral functioning of children raised in institutions has shown that these children are at substantial risk in various domains of functioning, including their physical[1], general behavioral (BakermansKranenburg et al., 2012; The St. Petersburg-USA Orphanage Research Team, 2008), cognitive[2], and neurophysiological[3]development. In terms of socio-emotional development, the predominant attachment classification among these infants is disorganized, because they have extremely limited opportunities for developing selective attachments with people.[4]
The research has suggested that the adverse developmental and behavioral functioning of institutionalized children depends on pre-institutional risk factors (The St. Petersburg-USA Orphanage Research Team, 2005; Van IJzendoorn et al., 2011), the quality of care in the institution[5], and the length of time the children spent in the institutional environment (Julian, 2013; Rutter et al., 2007). Studies have examined the role of the timing of institutionalization in studies of children transferred from institutions to adoptive families, and have shown associations between the time spent in the institution (age at adoption), and the subsequent developmental and behavioral functioning of post-institutional children (Kreppner et al., 2007; Merz & McCall, 2010; Muhamedrahimov et al., 2014). Problems are more likely to occur among children from more severely depriving institutions, and those children with a substantial history of institutional care (between 6 and 24 months depending on institutional conditions) and placement into post-institutional families at older ages (Hawk & McCall, 2011; Julian, 2013). In general, the results suggest that across most domains of development, institutional care which is limited to the first four to six months of life is not associated with a significantly increased risk for long-term adverse effects relative to non-institutionalized children (Zeanah et al., 2011).
Although these studies show that the exposure to institutional environments can increase the risk of later adverse developmental outcomes, they do not examine the early developmental pattern of delay in relation to the length of time in the institution, especially for those who were institutionalized in the first months of life. There has been no information on the behavioral development of the first year of life infants within the institutional period depending on their risk group (biological or no biological risk) and the type of caregiving environment in the institutions.
Length of Time in Institution
Since many factors might confound the development of institutionalized children (for example, age at intake, age at assessment, disability status, etc.), an analysis of the developmental and behavioral functioning of institutionally-raised children as a function of the time they spent in an institution would ideally be based on longitudinal assessments of the same group of children over their institutional residency; however, such assessments are rare. Instead, most studies compare the development of institutionalized with non-institutionalized children.
The early studies of the developmental consequences of institutional care on infants in their first year showed that demonstrable impairment was not observed in children under three months, but severe disturbances could be observed in those who had been institutionalized for more than eight months during their first year (Durfee 8c Wolf, 1933). It was found that, in contrast to children institutionalized at two or three years of age, who could be remediated to some extent, those institutionalized during their first year seemed unable to be remediated (Lowrey, 1940). The first longitudinal study of early institutionalized children found that at the end of the first year, children from a “foundling home” showed manifestations of negative environmental influences for development, namely, severe developmental retardation and deviant behavior patterns (Spitz, 1945), as compared to peers from parental home environments, and from a nursery for children of socially maladjustment and delinquent mothers.
The results of subsequent studies have both supported and contradicted these early data. For example, a study of infants in a Romanian orphanage showed that at an average of 6.5 months of age (with an average of 4.7 months of residence in the orphanage), children were already about three or four months behind the Denver II norms on all developmental variables (Sparling, Dragomir, Ramey, 8c Florescu, 2005). After an additional 12 months exposure to the institutional environment, the development of children had dropped to about seven months behind the Denver II norms, while the development of the experimental group exposed to an educational intervention program was still between three and four months behind.
In a study of orphaned Romanian children between the ages of 23 and 50 months, all children exhibited deficits in cognitive and social functioning. The majority were severely delayed, but their deficits were not related to age at entrance, or the length of time in the orphanage (Kaler 8c Freeman, 1994). A group of children 12-31 months of age raised in Romanian institutions exhibited serious disturbances of attachment, but there was no relationship between the length of institutionalization and their exhibiting signs of either emotionally withdrawn/inhibited or indiscriminately social/ disinhibited reactive attachment disorder (Zeanah et al., 2005). Thus, results of these subsequent studies are contradictory: some of them confirm that longer exposure to institutional environment leads to greater deficiencies, and others do not.
Length of Exposure to Interventions in Institutions
Studies have shown that interventions in institutions aimed at improving the quality of the institutional environment and care, have positive effects on different domains of childrens behavioral functioning[6]. It was found that the first positive changes in the behavior of institutionalized children can be observed after three months of exposure to an intervention program (Groark, Muhamedrahimov, Palmov, Nikiforova, 8c McCall, 2005). Institutionalized children tended to improve developmental^ and behaviorally on standardized infant tests after four to nine months of exposure to the training and structural changes intervention program, and continued to improve on many measures of physical growth, behavioral development, and social and emotional behavior after 9+ months of intervention (The St. Petersburg-USA Orphanage Research Team, 2008). These results were based on the analysis of children representing a wide age range. Additional study is needed to understand the effect of time in typical and post-interventional institutions on the development of children during their first months of life. It is notable that developmental and behavioral improvements after four to nine months of exposure to the institutional intervention program have been observed for children with disabilities, as well as for infants and young children with typical development. To the best of our knowledge, the above mentiones study is the only one on the effect of the length of exposure to institutional interventions on the development of children with disabilities.Thus, the literature suggests that there are inconsistent results on the association between the length of institutionalization and the development of resident children. Some studies have shown associations between the time spent in the institutional environment and developmental and behavioral functioning of children in institutions, whereas some have not shown such associations. The differences in findings may be because of differences in the institutional environments, ages at assessments, pre-institutional life experiences, and areas of child development (Hawk & McCall, 2011; Julian, 2013; Chernego & Muhamedrahimov, 2014). Our study attempts to resolve the discrepancy between studies finding no effect of time spent in institutions, and those studies finding an effect of time spent in institutions. It is aimed at examining the association between time spent in typical socialemotionally depriving Russian institutions, and the development of infants during the first year of life, including those with at biological risk of developmental delay.
Current Study
The main aim of our study was to examine the general behavioral development of infants living in institutions located in the Russian Federation between three and nine months of life, as a function of their birth circumstances and the nature of the care provided in the institution. We examined behavioral development longitudinally in threeto nine-months-old fulland preterm infants from two St. Petersburg institutions serving children from birth to four years of age (called Baby Homes) which had different caregiving environments: one typical of traditional Russian BHs (i.e., typical non-intervention Baby Home=NoI BH), and one in which a training and structural changes (T+SC BH) program of intervention was implemented (The St. Petersburg-USA Orphanage Research Team, 2005, 2008; Solodunova, Palmov, & Muhamedrahimov, 2017).
Our research interest in the group of preterm infants (30 to 36 weeks of gestation) was informed by several factors. First, according to WHO data, the preterm birth rate is dramatically and consistently rising (World Health Organization, 2015) with the moderate and late gestational age groups accounting for most of this increase (Talge, Holzman, Van Egeren, Symonds, Scheid, Senagore, & Sikorskii, 2012). Nearly one-third of children from St. Petersburg orphanages included in this study are preterm, with most being moderate and late preterm without medical complications. Second, despite being born toward the end of the preterm period and considered low-risk infants, this group of moderate and late preterm children is characterized by neurobehavioral immaturity and continues to be vulnerable to postnatal environmental conditions (Kinney, 2006; Nepomnyaschy et al., 2012). Third, it is well established that family-based early intervention programs have a strong positive effect on premature infants' development1, but there is a lack of information on the effect of a family-like environment in an institutional setting on a preterm infant's development.
We focused on the general behavioral development of BH infants and posed several questions. First, we examined whether the development of the infants declined between three and nine months of life in the typical NoI BH. We expected that several months of institutionalization in the traditional NoI BH would have deleterious effects on infants' development during the first months of life. Second, we examined whether infants in the T+SC BH would improve, rather than decline, in terms of behavioral development over time. Third, since both NoI and T+SC BHs included both preand full-term infants, we tested possible differences in the association between children's general behavioral development across age as a function of gestational age. Since there were large differences between typically developing children and those with disabilities in T+SC BH (The St. Petersburg-USA Orphanage Research Team, 2008), and the amount of improvement was greater for typically developing children, we expected that T+SC intervention would have a different effect on prevs full-term infants.
Method
This study used data from an intervention conducted in St. Petersburg, Russian Federation (The St. Petersburg-USA Orphanage Research Team, 2008), the report of which provides extensive methodological details that will not be repeated here.
Participants
Our analyses were based on the St. Petersburg BH intervention project database. For the purposes of the current study, those children who met the following criteria were selected: the availability of BH records on their birth information, including gestational age; no pathological symptoms of the central nervous system; no severe hereditary and somatic diseases; and complete assessments at three and nine months of age. The total group of 58 children included full-term children (FCh, N=36) with gestational ages of 37-41 weeks, and preterm children with gestational ages of 30-36 weeks (PCh, N=22). The birth information, including gestational age, was obtained from BH records. According to the type of BH intervention (NoI, T+SC) and their gestational age (pre-term and full-term), the children were divided into four groups: 1) full-term children from BH with no intervention program (FCh NoI, N=21); 2) preterm children from BH with no intervention (PCh NoI, N=12); 3) full-term children from BH after intervention program with family-like environment (FCh T+SC, N=15); and 4) preterm children from BH after intervention program with a family-like environment (PCh T+SC, N=10).
Table 1 presents the study sample's characteristics (means, standard deviations, and range). The characteristics of the preterm and full-term children were significantly different based on Preor Full-Term x Intervention Condition (NoI, T+SC) analyses of variance. There were no differences in the proportion of boys and girls within each group, so gender was ignored in the analyses. The age at which preterm children entered an institution was significantly older than for full-term children from both institutions, because usually preterm children spend more time in the hospital before entering an institution. There were no effects of Intervention Conditions (NoI and T+SC) on gestational age, birth weight, and age at the time of entering in the BH, but a significant effect for time in the BH by the time of assessment at the age of three, as well as nine months (see Table 1).
Table 1
Sample Characteristics
|
Measure |
Groups |
|
|
|
|
NoI (N=33, 22 males) |
T+SC (N=25,12 males) |
|||
|
PCh NoI (N=12; 8 males) |
FCh NoI (N=21; 14 males) |
PCh T+SC (N=10; 6 males) |
FCh T+SC (N=15; 6 males) |
|
|
Gestational age, weeks FPCh-FCh (1, 54) = 185.2, p < .001 |
37.5 (2.6) |
37.6 (2.9) |
||
|
|
F (1, 54) = 0.1, n.s |
|
||
|
34.7 (1.7) (30–36) |
39.1 (1.2) (37–40) |
34.4 (1.5) (31–36) |
39.7 (0.9) (38–41) |
|
|
F (1, 54) = 88.8, p < .001 |
F (1, 54) = 96.7, p < .001 |
|||
|
Birth weight, grams FPCh-FCh (1, 54) = 76.9, p < .001 |
2746(543) |
2830(737) |
||
|
|
F (1, 54) = 0.5, n.s |
|
||
|
2215 (254) (1680–2590) |
3049 (413) (2240–3770) |
2141(429) (1460-2850) |
3289 (498) (2601-4100) |
|
|
F (1, 54) = 31.0, p < .001 |
F (1, 54) = 46.1, p < .001 |
|||
|
Age at entering in institution, days FPCh-FCh (1, 54) = 9.7, p < .05 |
33(15) |
35 (16) |
||
|
|
F (1, 54) = 0.1, n.s |
|
||
|
40(11) (24-59) |
29(16) (5-72) |
43 (15) (16-66) |
29 (15) (7-57) |
|
|
F (1, 54) = 4.7, p < .05 |
F (1, 54) = 5.1, p < .05 |
|||
|
Time in BH by assessment at the age of 3 months, days FPCh-FCh (1, 54) = 13.7, p < .001 |
72 (17) |
59 (16) |
||
|
|
F (1, 54) = 7.3, p < .05 |
|
||
|
58 (13) |
81 (14) |
55 (15) |
62 (17) |
|
|
(37-84) |
(42-95) |
(26-78) |
(29-89) |
|
|
F (1, 54) = 17.8, p < .001 |
F (1, 54) = 1.4, n.s |
|||
|
Time in BH by assessment at the age of 9 months, days FPCh-FCh (1, 54) = 39.0, p < .05 |
256 (22) |
|
240 (16) |
|
|
|
F (1, 54) = 10.8, p < .001 |
|
||
|
234(13) |
268(15) |
231 (12) |
246 (16) |
|
|
(212-252) |
(224-283) |
(215-254) |
(223-272) |
|
|
F (1, 54) = 43.1, p < .001 |
F (1, 54) = 6.4, p < .05 |
|||
Procedure
Intervention. The two Baby Homes that participated in the current study (NoI and T+SC) belong to the health care system, and are considered to achieve acceptable standards for meeting children's basic medical and nutritional needs. Both participated in a large study conducted in St. Petersburg, Russian Federation (The St. Petersburg-USA Orphanage Research Team, 2008). The typical NoI BH is characterized by socio-emotional deficiencies, and business-like and perfunctory routine caretaking activities (Muhamedrahimov, 2000; The St. Petersburg-USA Orphanage Research Team, 2005). By contrast, the T+SC BH was involved in programs for training and structural changes interventions in which caregivers were trained to engage in sensitive and responsive interactions with the children. In addition, structural changes were implemented to reduce the number of different caregivers the children experienced, and to increase caregiver stability. They included a reduction in group size, the assignment of permanent primary caregivers to each group, integration of children by age and by disability status, and no transitions of children to new wards.
Assessment and procedure. The Battelle Development Inventory (BDI; (LINK Associates, 1988) was used to assess the children's developmental skills. The BDI includes a Total Score based on subscales for Personal-Social, Motor, Adaptive, Communication, and Cognition. Raw scores were converted to developmental quotients (DQs) based on a U.S. standardization study (LINK Associates, 1988). The BDI was administered in a special quiet room in each BH by independent assessors with psychological training, to individual children accompanied by the caregiver who knew the child best, or had the best relationship with the child (see The St. Petersburg-USA Orphanage Research Team, 2008). In the larger project, children were assessed periodically at different ages; the current study includes all those children who had BDI assessments at approximately three months (3.1±0.3, from 2.7 to 4.0 months) and nine months of age (9.2±0.2, from 8.5 to 9.5 months). The chronological age, not age from conception, was used for all children.
Results
Table 2 presents the means, standard deviations, and statistical results for the BDI Total DQs as a function of age, gestational age, and types of institutional care. Repeated analyses of variance were conducted on the BDI Total Scores in relation to Age (3 months, 9 months) x Gestational Age (preterm, full-term) x Type of Institutional Care (NoI, T+SC). Simple effects tests were then conducted to test the difference between the assessments at the two ages within each group of children. The BDI means are graphed in Figure 1 for each group (PCh NoI; FCh NoI; PCh T+SC; and FCh T+SC).
Table 2
Mean (Standard Deviations) BDI Total DQs and Comparisons
|
|
Time 1 |
Time 2 |
|
Nol |
86.3 (8.5) |
72.7 (9.3) |
|
F(1, 54) = 34.8, p < .001, η2 = .39 |
||
|
PCh Nol |
81.9 (7.4) |
69.8 (7.2) |
|
F(1, 54) = 11,30, p = .001, η2 = .17 |
||
|
FCh Nol |
88.8 (8.1) |
74.2 (10.1) |
|
F(1, 54) = 28.39, p < .001, η2 = .34 |
||
|
T+SC |
84.0 (11.1) |
91.0(12.1) |
|
F(1, 54) =5.9 , p = .018, η2 = .10 |
||
|
PCh T+SC |
81.7(11.3) |
84.4(14.0) |
|
F (1, 54) = 0.47, n.s. |
||
|
FCh T+SC |
85.6 (11.0) |
95.3 (8.7) |
|
F(1, 54) = 9.17, p = .004, η2 = .15 |
||
The main results of interest were a significant age effect: F(1, 54) = 4.32, p = .042, η2 = .07, and an Age x Type of Institutional Care interaction, F(1, 54) = 32.95, p<.001, η2 = .38. There were no significant interaction effects for Age x Gestational Age, F(1, 54) = .47, n.s., and Age x Type of Institutional Care x Gestational Age, F(1, 54) = 1.93, n.s., which indicated that the Age x Type of Institutional Care developmental changes were not significantly different for children in each gestational age group. Thus, there was a significant decline of the BDI Total DQs from three to nine months for children from the NoI BH, but a significant improvement in BDI Total DQs for children from the T+SC BH. Although the three-way interaction was not significant, Table 2 and Figure 1 suggest that the improvement among T+SC children was significant for FCh, but not for PCh group.
There were two additional main effects: One was for Gestational Age: F(1, 54) = 10.2, p = 0.002, η2 = 0.16, in which the FCh had higher means than the PCh group. The other was for the type of Institutional Intervention: F(1, 54) = 15.6, p < 0.001, η2 = 0.22, in which children from T+SC BH displayed higher scores than children from NoI BH. The interaction between these factors was not significant F(1, 54)<1, n.s., indicating that the preterm/full-term differences were not different within each institution.
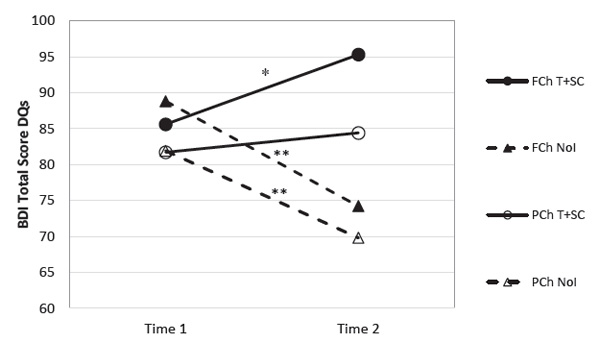
Figure 1. Longitudinal Battelle Developmental Inventory (BDI) developmental quotients (Total Score DQS) for two interventional conditions (NoI, T+SC) and gestational status (PCh, FCh) as a function of time; asterisks (*=p<.05, **=p<.001) indicate significant change in BDI Total Score DQs during that assessment interval.
Discussion
The current study focused on a subsample of infants three to nine months of age from two St. Petersburg (Russian Federation) Baby Homes serving children from birth to four years of age. The infants were adequately cared for medically and with respect to nutrition, but deficient in caregiver-child interactions (The St. PetersburgUSA Orphanage Research Team, 2008). One BH received training and structural changes designed to improve the quality of caregiver-child interactions (T+SC), and the other received no such intervention (NoI). The main aim of the study was to examine the general behavioral development of institutionalized infants between three and nine months of age, as a function of the type of Institutional Intervention (T+SC or NoI) and the children's Gestational Age (born preterm at 30-36 weeks or full-term at 37-41 weeks). The primary questions were whether the intervention caused a change in the child's developmental change between three and nine months of age, and whether that change was the same for preterm and full-term infants.
Children in the traditional NoI BH displayed significant declines in BDI Total DQs during the six months between three and nine months of age. These results are consistent with previous study results which showed developmental deficits in institutionalized children within the first year of life, ranging from an average of 4.7 months (from the very early study of infants in orphanages; Durfee & Wolf, 1933) to eight months (from the study of children in the Romanian orphanage; Sparling et al., 2005) in the orphanage. A meta-analysis has shown that institutionalized infants in the first year of life score below infants raised by their parents (Van IJzendorn, Luijk, Juffer, 2008), and that can be associated with their birth circumstances and their level of development when they entered the institution (The St. Petersburg-USA Orphanage Research Team, 2005). Additionally, the current study shows that the developmental decline in infants in the first year of life depends on the institutional environment: The exposure to the socio-emotional depriving conditions of a Russian Baby Home can lead to intra-individual developmental decline in infants aged three to nine months, and these declines are shown by both full-term and preterm infants.
Children in the Baby Homes with T+SC programs showed a significant improvement in Total DQs between the ages of three and nine months. These results reveal that, in contrast to the negative effect on children's development of the typical traditional social-emotionally depriving institution, exposure to the caregiving environment not only prevents the decline, but promotes the infants' development in the first year of life. Generally, infants observed at three and nine months of age from the T+SCh BH conditions displayed higher developmental scores than their peers from the NoI BH, and these results suggest that the improvement observed in the larger study for children of a broader age range (The St. Petersburg-USA Orphanage Research Team, 2008) also applies to infants in their first year of life. Thus, a relatively short period of seven to nine months exposure to the socially-emotionally depriving institutional environment leads to infants' developmental decline, while the same length of exposure to a T+SC caregiving environment leads to improvements. In general, the group of preterm children had lower mean BDI Total DQs than the full-term children. These findings are consistent with the recent studies that have shown the persistence through infancy of developmental delays and negative neurodevelopmental outcomes among preterm children (Eickmann, Malkes, & Lima, 2012; Vohr, 2013; Platt, 2014; Natarajan, & Shankaran, 2016). This might be explained by the fact that preterm birth dramatically interrupts the development of the brain during the third trimester of pregnancy (Kinney, 2006; McGowan et al., 2011; Duerden, Taylor, & Miller, 2013).
The significant developmental improvement of the infants receiving the T+SC intervention between the ages of three and nine months was somewhat stronger for full-term than for preterm infants. Previous studies of children in T+SC BH demonstrated developmental differences between children with disabilities and typically developing children, and that while those with disabilities gained, the improvement was not as much as for typically developing children (The St. PetersburgUSA Orphanage Research Team, 2008). The results of the current study are quite consistent with this finding, and confirm that this trend is true for preterm children without certain obvious disabilities.
There are several possible reasons for this difference. First, the greater variability of individual developmental trajectories of preterm infants could mask or postpone the positive effects of the intervention programs (Engle, Tomashek, & Wallman, 2007; Guillois et al., 2012; McGowan et al., 2011). Furthermore, immature organisms could require longer exposure to the family-like environment, because more prolonged experience with stable and nurturing caregiving is needed for positive developmental outcomes. This is consistent with research showing improvements in the general behavioral functioning of preterm children after nine or 12 months of an intervention program [1].
Second, it is well established that the heightened vulnerability of immature organisms to environmental conditions requires implementation of individualized developmental care programs, in which early social-emotional caregiving interactions are combined with structured and highly differentiated inputs (Aucott, Donohue, Atkins, & Allen, 2002; Phillips, 2013). We assume that an additional early intervention program is necessary in the institutional settings to meet the individual developmental needs of pre-term children as well as those from other biological risk groups.
Practical Implications
The results of this study have practical implications. First, the research findings highlight a crucial need of children left without parental care in a family environment. Although the Russian government has emphasized family care alternatives for institutionalized children, it will take time to implement these procedures, and many children, especially those with disabilities, will be institutionalized for many years before these provisions are carried out.
The special resolution of the Russian government (issued 24/05/2014) does stipulate the creation of institutions with family-like environments, the elimination of periodic transitions of children to new wards, and the establishment of primary caregivers (The Resolution of the Government of the Russian Federation No. 481, 2014). However, that resolution does not provide for caregiver training that is focused on child development and warm, sensitive, responsive caregiverchild interaction. Our research has shown persuasively that only comprehensive intervention, consisting of both structural changes and training of caregivers, can produce significant results, and that such intervention has positive developmental effects for both children with disabilities and those with typical development (The St. Petersburg-USA Orphanage Research Team, 2008).
Second, our research indicated that even children who are preterm without certain obvious disabilities are at higher risk for delayed development, at least in their first nine months. Perhaps an additional early intervention program should be created for them. Such a program should take into consideration the specific needs of individual children, and be an essential supplement to the general program directed to fulfilling children's needs in a sensitive, responsive, and stable caregiving environment.
Conclusion
The current study showed that both full-term and preterm children from the typical socio-emotionally depriving, non-intervention institution (Baby Home) showed significant developmental declines between three and nine months of age, as measured in Battelle Development Inventory Total scores, whereas full-term children in a Baby Home where staff had undergone a training plus structural changes intervention program, improved over this period of time. In general, the group of fullterm children had higher mean BDI Total DQs than the preterm group, and children from the Baby Home with the intervention program displayed higher scores than children from the non-intervention one. Thus, the current study showed that ral development of infants, depends both on the type of institutional care environment as well as the gestational age of the children.
Limitations
This study had a number of limitations. First, the sample size of children observed at three and nine months of age was small. This was due to the fact that children housed in orphanages in their first months of life are mostly those who have pathological symptoms of the central nervous system and severe hereditary and somatic diseases; accordingly, the number of healthy children is somewhat small. Another factor was that healthy children of this age are the most attractive for adoption, and therefore often do not stay in the institution long enough to provide full longitudinal data.
Second, the intervention consisted of general training of caregivers on providing sensitive and responsive interactions, not on specific actions and techniques. This approach has the benefit of encouraging caregivers to adjust their behavior to fit children of different ages, but the disadvantage of not providing more specific intervention programs and techniques to match individual children's unique status, especially those with disabilities.
Third, it is possible that the general developmental change during the seven to nine months of institutionalization in the group of preterm children may not be the same or similar as that of children from other biological risk groups. However, the research data from a large intervention project showed a positive effect of the intervention on a wide group of children with disabilities, and the negative influence of a traditional orphanage environment on the development of children (The St. Petersburg-USA Orphanage Research Team, 2008). Acknowledgment
This study was funded by grant HD39017 from the Eunice Shriver Kennedy National Institute of Child Health and Human Development (to R.B. McCall and C.J. Groark). The analyses and preparation of the paper was supported by grant 14.W01.17.460-MK from the President of the Russian Federation for governmental support of young Russian researchers (to D.I. Chernego). The interpretations presented in this article are those of the authors, not the funder.
References
Als, H., Duffy, F. H., & McAnulty, G. B. (2004). Early experience alters brain function and structure. Pediatrics, 113(4), 846-857. https://doi.org/10.1542/peds.113.4.846
Aucott, S., Donohue, P. K., Atkins, E., & Allen, M. C. (2002). Neurodevelopmental care in the NICU. Mental Retardation and Developmental Disabilities Research Reviews, 8(4), 298-308. https://doi.org/10.1002/mrdd.10040
Bakermans-Kranenburg, M. J., Bunkers, K. M., Dobrova-Krol, N. A., Engle, P., Fox, N. A., Gamer, G., … & Zeanah, C. H. (2012). The Development and care of institutionally raised children. Child Development Perspectives, 6(2), 174-180. https://doi.org/10.1111/j.17508606.2011.00231.x
Bakermans-Kranenburg, M. J., van IJzendoorn, M. H., & Juffer, F. (2008). Earlier is better: A meta-analysis of 70 years of intervention improving cognitive development in institutionalized children. Monographs of the Society for Research in Child Development, 73(3), 279-93. https://doi.org/10.1111/j.1540-5834.2008.00498.x
Berument, S. K. (2013). Environmental enrichment and caregiver training to support the development of birth to 6-year-olds in Turkish orphanages. Infant Mental Health Journal, 34(3), 189-201. https://doi.org/10.1002/imhj.21380
Bick, J. & Nelson, C .A. (2016). Early adverse experiences and the developing brain. Neuropsychopharmacology, 41(1), 177-196. https://doi.org/10.1038/npp.2015.252
Chernego, D. I., Vasilyeva, M. J., Solodunova, M. Y, Nikiforova, N. V., Palmov, O. I., McCall, R. B. ..., & Muhamedrahimov, R. J. (2017). Mental development of preterm infants in different institutional environment. Psikhologicheskii zhurnal [Psychological Journal], 38(2), 55-65.
Chernego, D. I. & Muhamedrahimov, R. J. (2014). Comparative study of mental development of preterm and full-term infants in age 3 to 24 months raised in an orphanage. Psychological Journal, 35(4), 47-55.
Duerden, E. G., Taylor, M. J., & Miller, S. P. (2013). Brain development in infants born preterm: looking beyond injury. Seminars in Pediatric Neurology, 20(1), 65-74. https://doi. org/10.1016/j.spen.2013.06.007
Durfee, H. & Wolf, K. (1933). Anstaltspflege und Entwicklung im ersten Lebensjahr. Zeitschrift Fuer Kinderforschung, 42(3), 273-320.
Eickmann, S. H., Malkes, N. F. de A., & Lima, M. de C. (2012). Psychomotor development of preterm infants aged 6 to 12 months. Sao Paulo Medical Journal, 130(5), 299-306. https:// doi.org/10.1590/S1516-31802012000500006
Engle, W. A., Tomashek, K. M., & Wallman, C. (2007). "Late-preterm" infants: A population at risk. Pediatrics, 120(6), 1390–401. https://doi.org/10.1542/peds.2007-2952
Groark, C. J., Muhamedrahimov, R. J., Palmov, O. I., Nikiforova, N. V., & McCall, R. B. (2005). Improvements in early care in Russian orphanages and their relationship to observed behaviors. Infant Mental Health Journal, 26(2), 96-109. https://doi.org/10.1002/imhj.20041
Guillois, B., Castel, S., Beunard, A., Blaizot, X., Creveuil, C., & Proia-Lelouey, N. (2012). Effect of early intervention programs on the neurobehavioral outcome in premature infants after discharge. Archives de Pediatrie, 19(9), 990–997. https://doi.org/10.1016/j.arcped.2012.06.004
Güler, O. E., Hostinar, C. E., Frenn, K. A., Nelson, C. A., Gunnar, M. R., & Thomas, K. M. (2012). Electrophysiological evidence of altered memory processing in children experiencing early deprivation. Developmental Science,15(3), 345-358. doi:10.1111/j.1467-7687.2011.01131
Gunnar, M. (2001). Effects of early deprivation: Findings from orphanage-raised infants and children. In C.A. Nelson and M. Luciana (Ed.), Handbook of developmental cognitive neuroscience, 617-629. Cambridge, MA: MIT Press.
Hawk, B. N. & McCall, R. B. (2011). Specific extreme behaviors of postinstitutionalized Russian adoptees. Developmental Psychology, 47(3), 732-8. https://doi.org/10.1037/a0021108
Julian, M. M. (2013). Age at adoption from institutional care as a window into the lasting effects of early experiences. Clinical Child and Family Psychology Review, 16(2), 101-45. https://doi. org/10.1007/s10567-013-0130-6
Kaler, S. R. & Freeman, B. J. (1994). Analysis of environmental deprivation: Cognitive and social development in Romanian orphans. Journal of Child Psychology and Psychiatry, 35(4), 769781. https://doi.org/10.1111/j.1469-7610.1994.tb01220.x
Kinney, H. C. (2006). The near-term (late preterm) human brain and risk for periventricular leukomalacia: A review. Seminars in Perinatology, 30(2), 81-88. https://doi.org/10.1053/j. semperi.2006.02.006
Kreppner, J. M., Rutter, M., Beckett, C., Castle, J., Colvert, E., Groothues, C., … & Sonuga-Barke, E. J. S. (2007). Normality and impairment following profound early institutional deprivation: A longitudinal follow-up into early adolescence. Developmental Psychology, 43(4), 93146. https://doi.org/10.1037/0012-1649.43.4.931
Landry, S. H., Smith, K. E., & Swank, P. R. (2006). Responsive parenting: Establishing early foundations for social, communication, and independent problem-solving skills. Developmental Psychology, 42(4), 627-42. https://doi.org/10.1037/0012-1649.42.4.627
Lassi, Z. S., Middleton, P. F., Crowther, C., & Bhutta, Z. A. (2015). Interventions to improve neonatal health and later survival: an overview of systematic reviews. EBioMedicine, 2(8), 985-1000. https://doi.org/10.1016/j.ebiom.2015.05.023
LINK Associates. (1988). The Battelle Developmental Inventory scoring booklet. Itasca, IL:Riverside.
Lomann, M. M., Jonson, A. E., Westerlund, A., Pollack, C. D., Nelson, C. A., & Gunnar, M.R. (2013). The effect of early deprivation on executive attention in middle childhood. Journal of Child Psychology and Psychiatry, 54(1), 37-45. https://doi.org/10.1111/j.14697610.2012.02602.x
Lowrey, L. G. (1940). Personality distortion and early institutional care. American Journal of Orthopsychiatry, 10(3), 576-585. https://doi.org/10.1111/j.1939-0025.1940.tb05725.x
Marshall, P. J., Fox, N. A., & the BEIP Core Group. (2004). A comparison of the electroencephalogram between institutionalized and community children in Romania. Journal of Cognitive
Neuroscience, 16(8), 1327-1338. https://doi.org/10.1162/0898929042304723 McCall, R. B., Groark, C. J., Fish, L. A., Harkins, D., Serrano, G., & Gordon, K. (2010). A socioemotional intervention in a Latin American orphanage. Infant Mental Health Journal, 31(5), 521-542. https://doi.org/10.1002/imhj.20270
McGowan, J. E., Alderdice, F. A., Holmes, V. A., & Johnston, L. (2011). Early childhood development of late-preterm infants: A systematic review. Pediatrics, 127(6), 1111-1124. https://doi. org/10.1542/peds.2010-2257
McLaughlin, K A., Sheridan, M. A., & Lambert, H. K. (2014). Childhood adversity and neural development: Deprivation and threat as distinct dimensions of early experience. Neuroscience & Biobehavioral Reviews 47, 578-591. https://doi.org/10.1016/j.neubiorev.2014.10.012
Merz, E. C. & McCall, R. B. (2010). Behavior problems in children adopted from psychosocially depriving institutions. Journal of Abnormal Child Psychology, 38(4), 459-70. https://doi. org/10.1007/s10802-009-9383-4
Myers, M. M., Grieve, P. G., Stark, P. I., Isler, J. R., Hofer, M. A., Yang, J., … & Welch, M.G. (2015). Family nurture intervention in preterm infants alters frontal cortical functional connectivity assessed by EEG coherence. Acta Paediatrica 104, 670-677. https://doi.org/10.1111/ apa.13007
Muhamedrahimov, R. J. (2000). New attitudes: Infant care facilities in St. Petersburg, Russia. In J. D. Osofsky & H. E. Fitzgerald (Eds.), WAIMH handbook of infant mental health. Vol. 1. Perspectives on infant mental health (pp. 245-294). New York, NY: Wiley.
Muhamedrahimov, R. J., Agarkova, V. V., Vershnina, E. A., Palmov, O. I., Nikiforova, N. V., Mc-Call, R. B., & Groark, C. J. (2014). Behavior problems in children transferred from a socioemotionally depriving institution to St. Petersburg (Russian Federation) families. Infant Mental Health Journal, 35(2), 111-122. https://doi.org/10.1002/imhj.21435
Muhamedrahimov, R. J., Arintcina, I. A., Solodunova, M. Y., Anikina, V. O., Vasilyeva, M. J., Chernego, D. I., … & Grigorenko, E. L. (2016). Structural Characteristics of Institutional Environment for Young Children. Psychology in Russia: State of the Art, 9(2), 103-112. https://doi.org/10.11621/pir.2016.0307
Notes
1. Van Ijzendoorn, Bakermans-Kranenburg, & Juffer, 2007; Warner, McCall, Groark, Kim, Muhamedrahimov, Palmov, & Nikiforova, 2017.
2. Nelson, Zeanah, Fox, Marshall, Smyke, & Guthrie, 2007; Van Ijzendoorn et al., 2011; Giiler, Hostinar, Frenn, Nelson, Gunnar, & Thomas, 2012; Lomann, Jonson, Westerlund, Pollack, Nelson, & Gunnar, 2013; Vasilyeva, Korshina, Kurohtina, Vershinina, Kornilov, Muhamedrahimov, & Grigorenko, 2017.
3. Marshall, Fox, & the BEIP Core Group, 2004; McLaughlin, Sheridan, & Lambert, 2014; Bick & Nelson, 2016.
4. Bakermans-Kranenburg et al., 2012; The St. Petersburg-USA Orphanage Research Team, 2008; Zeanah, Smyke, Koga, Carlson, & the BEIP Core Group, 2005.
5. Gunnar, 2001; Merz & McCall, 2010; Muhamedrahimov, Arintcina, Solodunova, Anikina, Vasilyeva, Chernego, Tsvetkova, & Grigorenko, 2016; Chernego, Vasilyeva, Solodunova, Nikiforova, Palmov, McCall, Groark, & Muhamedrahimov, 2017.
6.Bakermans-Kranenburg, van IJendoorn, & Juffer, 2008; Berument, 2013; McCall, Groark, Fish, Harkins, Serrano, & Gordon, 2010; The St. Petersburg-USA Orphanage Research Team, 2008.
To cite this article: Muhamedrahimov R.J., Chernego D.I., Vasilyeva M.J., Palmov O.I., Vershinina E.A., Nikiforova N.V., McCall R.B., Groark C.J. (2018) Developmental Change in Full- and Preterm Infants between the Ages of Three and Nine Months in Institutions with Different Caregiving Environments. Psychology in Russia: State of the Art, 11 (3), 152-167
The journal content is licensed with CC BY-NC “Attribution-NonCommercial” Creative Commons license.







