Rehabilitation of semantic aphasia in spanish speaking patient
Solovieva, Yu.  Autonomous University of Puebla, Puebla, Mexico
Autonomous University of Puebla, Puebla, Mexico
Abstract
Background. Aphasia is defined as a language disorder resulting from brain damage. The establishment of the relationship between the assessment and the procedures for rehabilitation is one of fundamental aspects of clinical neuropsychology.
Objective. The objective of this study is to describe the case of a Spanish-speaking patient with semantic aphasia, along with the strategies used in her neuropsychological assessment, and the procedures and results of her rehabilitation.
Design. The study method consisted of a clinical “Case Study” through qualitative neuropsychological syndrome analysis during pre- and post-assessment. The program for rehabilitation was designed especially for this case, and applied in individual therapeutic sessions with the patient. The inclusion of different kinds of material, perceptual, and verbal tasks permitted the patient to follow the levels of formation of actions with spatial orientation, starting from the most concrete level, and passing on to a more general, abstract level. The process of rehabilitation was carried out as a joint activity, taking into account the patient’s motivation and personality.
Results. Important positive changes were obtained by the time of the final assessment. The patient became able to understand complex grammatical structures in sentences and texts, in order to fulfill construction tasks and to express herself correctly both orally and in writing.
Conclusion. The authors conclude that an effective assessment leads directly to the effectiveness of the whole process of elaborating and realizing rehabilitation. Semantic aphasia can be studied in Spanish-speaking patients by using the qualitative methodology of neuropsychological assessment proposed in the works of A.R. Luria.
Received: 11.02.2017
Accepted: 05.04.2017
Themes: Psychology and culture
PDF: http://psychologyinrussia.com/volumes/pdf/2018_1/psych_1_2018-11_Solovieva.pdf
Pages: 137-150
DOI: 10.11621/pir.2018.0111
Keywords: aphasia, semantic aphasia, diagnosis of aphasia, neuropsychological rehabilitation, brain injury
Introduction
Aphasia is commonly defined as a language disorder resulting from brain damage (Benson & Ardila, 1996), or as an alteration of the ability to communicate due to circumscribed injuries (Hecaen, 1979). However, it is not always clear what the basis for these alterations is. Are those alterations a system which includes different kinds of speech defects only, or does it include diverse mental operations?
Apparently, the point of view that there are different types and syndromes of aphasia is a predominant one (Goodglass & Kaplan, 1972; Kertesz, 1979; Ardila, 2010), and is used by the authors when considering assessment and classification. At the same time, proposals for differentiated rehabilitation for different types of aphasia are not very common. Normally, articles on the topic of rehabilitation are directed to aphasia in general (Moreno & Blanco, 2000; Marini et al., 2007; Boo & Rose, 2011; Kiran et al., 2015), or even in a more general way to patients with brain injury (Lopez, 2001; Pulvermiiller & Berthier, 2008; Cherney et al., 2008; Rasquin, Welter, & Van Heugten, 2013; Harris & Olson, 2014; Smeets et al., 2017).
According to Lurias conception (1947), it is possible to classify aphasic syndromes according to the neuropsychological factors or mechanisms which determine the syndrome observed in each patient. A well-known example is the classification of types of aphasia(Luria, 1964; Lazaro, Quintanar, & Solovieva, 2010). Semantic aphasia is described as a specific neuropsychological clinical syndrome, or a kind of speech impairment, which can be observed in cases of brain damage in the posterior temporal parietal and occipital (TPO region) zones of both hemispheres. However, in the case of semantic aphasia, the phonic and phonemic level of language is preserved. No difficulties in either pronunciation or comprehension on the level of speech sounds (phonemes) can be observed. There are no defects of oral praxis or of the motor aspects of articulation. All the patients’ primary functions are also preserved. No specific mistakes can be observed on the level of isolated vowels or consonants, and even words. The meaning of frequent concrete words is preserved, as well as visual recognition of single objects.
On the other hand, severe defects in the logical and grammatical level of speech production and understanding can be found. The patients with this kind of aphasia manifest peculiar disturbances of language production and comprehension at the level of sentences and texts. The disturbances specific to semantic aphasia are expressed in the absence of access to complex grammatical structures which involve temporal, spatial, comparative, and causal relations, as well as genitive prepositions (possessives). Examples of such constructions might be: “Put the pencil under the book and upon the notebook”; “Show the picture in which you observe that the bird is on the right (left) side of the tree”; “Walk four steps forward and two back,” and so on. Such constructions are difficult for patients in both a written and oral modality. The patients have no access to de-codification of such types of sentences, nor can they use them in their own speech (Solovieva, Chavez, & Quintanar, 2001; Solovieva, Renteria, & Quintanar, 2001; Solovieva et al., 2001).
Such a phenomenon was described for the first time with respect to Russianspeaking patients in the works by A.R. Luria (Luria, 1973). A patient with semantic aphasia was famously described in Lurias bestseller “A man with a shattered world” (1972). Afterwards, similar cases were described and presented by neuropsychologists ofLurias school (Kogan, 1962; Tsvetkova, 1977, 1988; Glozman, 1999). The linguistic difficulties of patients with semantic aphasia could be described as grammatical disturbances, which are related to simultaneous disorganization of spatial orientation and perceptions. It is important to stress that if no such sentences were included in the neuropsychological assessment, the specialist might not notice any kind of aphasia at all, and would relate the patient s difficulties to problems of memory or logical processing (Solovieva, Chavez, & Quintanar, 2001). It is interesting that the patients themselves stress their memory defects, but not speech difficulties (Quintanar & Solovieva, 2001).
In order to accurately identify such problems, the neuropsychologist has to first have conceptual knowledge about the kinds of structures used in the patients specific language. Secondly, it is necessary to provide appropriate items for assessing the verbal sphere of patients with brain injury, and especially those with aphasia. Many well-known batteries of aphasia testing do not include such items (Boston). Probably there are no examples of such items for aphasia testing in English. As for Spanish authors, the examples are the Barcelona Test (Pena-Casanova, 2005); the Brief Neuropsychological Assessment for Adults (Quintanar & Solovieva, 2013); the Guide for Neuropsychological Diagnosis (Ardila & Ostrosky, 2011) and the Clinical Assessment of Aphasia (Quintanar, Solovieva & Leon-Carrion (2013).
For assessing oral production, we used the following example: “Our uncle had his breakfast after reading the newspaper. What did he do first?” (Quintanar & Solovieva, 2013).
During the assessment procedure it is useful to verify how successfully the patient understands complex verbal structures by presenting him or her with pictures with options. Some examples used during assessment in the Spanish language are: “In which picture can you see that the pupil of the teacher (teacher of the pupil) is writing on the board?”; “In which picture can you see that there are more orange flowers than white flowers in the vase?”; “In which picture do you see that the father of the son is giving a gift” (Quintanar, Solovieva, & Leon-Carrion, 2013). With this last example we wanted to show that not all spatial complex structures in one language (Spanish) are spatial complex structures in English or any other language. In the Spanish language, the construction “father of the son” and “son of the father” are spatially complex, but commonly used. In English, direct translation doesn’t show the level of structural complexity. That is why it is necessary to create language-specific items for neuropsychological assessment, instead of directly translating from one language to another. We believe that translating neuropsychological tests for assessment of aphasia is not a proper methodology (Goodglass, Kaplan, & Barresi, 1996).
Language difficulties are not the only troubles patients with semantic aphasia have. The patients also present severe difficulties in organizing conceptual writing at the level of sentences and text. Additionally, important problems with numeric operations, problem solving, and constructive abilities can commonly be detected. Such problems also occur in patients with “agraphia within aphasia,” and patients with logical (mental) processing or constructive disabilities, or parallel alterations of oral and written language (Balasurbramanian, 2005; Luria & Tsvetkova, 1979; Lazaro, Quintanar, & Solovieva, 2010). The absence of adequate testing procedures and knowledge of this kind of aphasia might lead to severe diagnostic errors. In linguistic contexts other than Russian, semantic aphasia frequently is not considered because the types of linguistic tests used are not directed to spatial organization of speech. Constructive problems, lack of spatial orientation, and numeric disorganization could be often considered as problems related to executive functions separately from language level (Luria, 1973; Solovieva, Chavez, & Quintanar, 2001; Lazaro, Quintanar, & Solovieva, 2010).
Objective
The objective of this study was to demonstrate the advantages and possibilities of the method proposed by A.R. Luria for analyzing aphasia in the case of a Spanishspeaking patient with semantic aphasia. At the same time, the study showed the necessity of a profound relationship between the strategies used for neuropsychological assessment and the procedures for rehabilitation.
Method
The study used the clinical “Case Study” method with qualitative neuropsychological syndrome analysis during preand post-assessment. The program for rehabilitation was designed specifically for this case, and applied in individual therapeutic sessions with the patient.
Case description
Our case was a 34 year old female patient, right-handed, with a formal education of 12 years in the Mexican educational system (technical level or high school), and a police officer by profession. The patient suffered brain injury by a bullet wound gotten during night duty. The patient had suffered severe CTE in the posterior bilateral cortical region. The patient temporarily manifested loss of smell and taste, loss of orientation in space, places, and temporal aspects, and memory problems. Primary perception was preserved for all modalities. The patient had a consultation with the Neuropsychological Service of University Hospital of the City of Puebla (Mexico). This clinical service is provided by the Masters Program on Neuropsychological Diagnosis and Rehabilitation of the Faculty of Psychology of Autonomous University of Puebla. The patient expressed the need for neuropsychological attention due to having serious difficulties in the process of writing, reading, comprehension of language, and general orientation.
Stages of study and procedure
The Neuropsychological Assessment was applied in five individual sessions of one hour each. After that, the Program of Neuropsychological Rehabilitation was created and applied in 37 individual sessions of one hour each over six months. At the end, another neuropsychological assessment was done, and the qualitative results were compared.
The initial Neuropsychological Assessment was carried out using instruments for qualitative neuropsycholgical assessment created for Spanish-speaking patients (Quintanar, Solovieva, & Leon-Carrion, 2011; Quintanar & Solovieva, 2013). These instruments included non-verbal tasks for phonemic discrimination, motor organization of praxis, and kinesthetic and visual perception of simple objects and images. The verbal tasks included items for assessing syntactic organization of sentences, word production and understanding, discrimination of sounds and syllables according to phonemic and kinesthetic analysis and synthesis, understanding of the sense of texts, and serial speech production. All the items were created by the authors according to the Lurias theory of functional brain organization in speech (Luria, 1973). Semantic, syntactic, and phonemic features of the Spanish language were considered (Quintanar & Solovieva, 2002; Quintanar, Solovieva, & Lazaro, 2006).
The initial Neuropsychological Assessment pointed out the conservation of the following mechanisms of the patient’s activity: phonemic discrimination, motor organization of praxis and speech, kinesthetic and visual perception of simple objects and images, programming and control of voluntary activity, and elementary retention in all modalities. Comprehension of common isolated sounds, syllables, words, and direct sentences, including orders with a simple structure, were preserved.
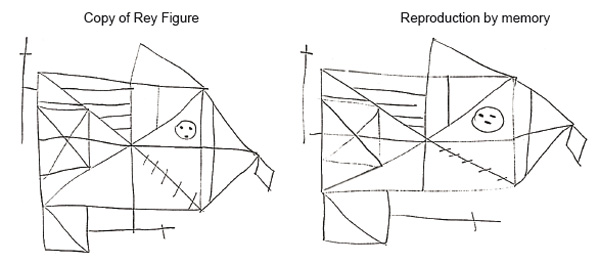
All kinds of complex tasks, which included simultaneous spatial synthesis and analysis, were especially difficult for the patient. Such difficulties were observed in the following tasks: construction (Kohs cubes); copying a Rey complex figure; comprehension of sentences and texts with a complex semantic structure (Show the picture in which the “dog is running behind the lady and in front of the car,” or “Who is the brother of your mother?” and so on). All sentences with that kind of semantic structure were not accessible to the patient. The solution of mathematical problems and examples, written speech production, and understanding of sentences and texts were inaccessible. On the basis of these clinical data, the neuropsychological diagnosis of semantic aphasia was established.
Figure 1 shows the copy of Rey figure, in which the patients severe difficulties with spatial organization can be observed.
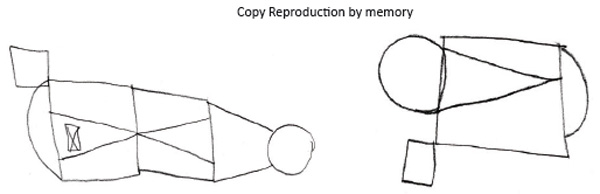
Figure 1. Task “Copy and reproduction by memory of Rey figure” before rehabilitation
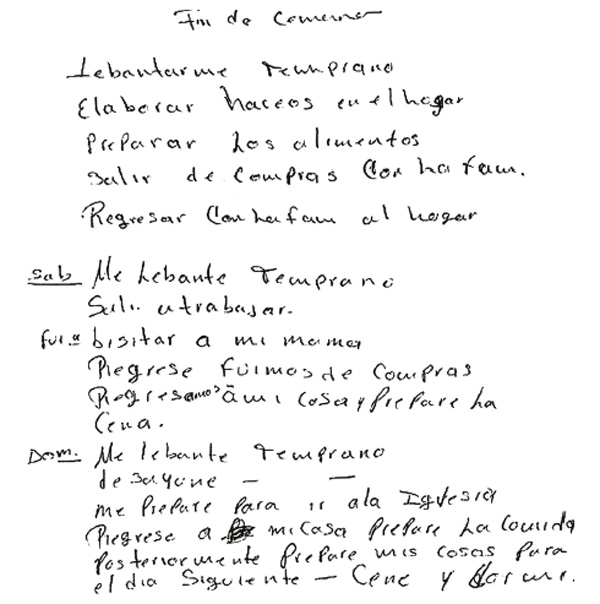
The patient showed severe difficulties in comprehending literary texts (stories read by the psychologist). The task of writing a little story of her choice, on the topic “My Day,” was too difficult for her (Figure 2).
Figure 2. Task “Free writing composition”
The patient has written: “I woke up, had breakfast. Talked to my daughter,” and has refused to go on.
Program for Neuropsychological Rehabilitation
The program for neuropsychological rehabilitation was designed according to the patients needs and potential, and the clinical picture of semantic aphasia (Quintanar, Lazaro, & Solovieva, 2009; Quintanar & Solovieva, 2016). The objective of the program was to provide gradual rehabilitation of spatial functions (simultaneous analysis and synthesis) on different levels of action: material, perceptual, and verbal. The material level included actions with real objects and their images, and construction tasks with blocks and cubes; the perceptual level included actions with symbols, signs, schemes, and maps; the verbal level was directed to production and comprehension of sentences with spatial and genitive prepositions. The second stage of the program was directed to patients production of proper texts with the help of the therapist. The final stage proposed working with arithmetic problems.
The structure of the action was always determined with respect to the patient s strong motivation for recovery, and the operations and conscious objectives of the actions which were attractive and accessible to the patient when accompanied by proper explanation and external help (Leontiev, 1983). All actions were completed with the assistance of a neuropsychologist who provided external objective, perceptual, and verbal help at all moments. Specific orientation was created for some intellectual tasks (Talizina, 2009; Solovieva, 2014). There was modification of the level of consciousness of spatial relations between material, perceptual, and verbal phenomena, according to the known practice of changing the purpose of external actions during rehabilitation (Leontiev, 2011). In the case of semantic aphasia, the actions chosen for rehabilitation should necessarily include operations with spatial relations. Automatic simultaneous subconscious operations were converted into sequential conscious step-by-step actions. All tasks were presented as joint actions with an external orientation by the neuropsychologist.
Below we show the stages of the program with examples of the tasks.
STAGE 1
Objective: Rehabilitation of the consciousness of spatial relations between objects, the patients own body, and her verbal reflection upon them.
Tasks:
-
Dialogue between the patient and therapist, including on aspects of spatial relations with objects in real space, pictures, and photographs. Constant usage of spatial prepositions: on my (your) left (right), between, in the middle, behind, after, before, in front of, outside, side by side, the first (last), the previous, the next to, the next, on, under, and so on. All prepositions were used as they are in conversational Spanish.
-
Usage of signs (symbols) to indicate the direction of an action: up, down, left, right. Constant reflective usage of prepositions and other spatial grammatical constructions (verbs and phrases).
-
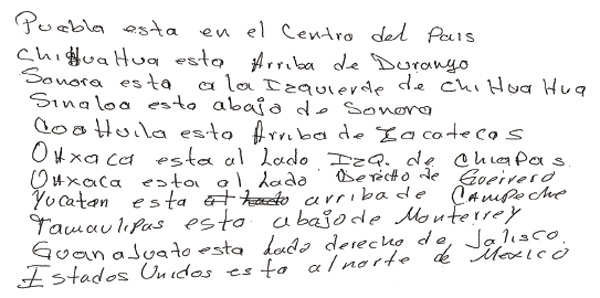
Work with geographic maps (birth City, Country, World political map). Identification of geographic objects (names) with the use of signs for South, North, East, West, Center. Creation of the relationship between such geographic notions and directions: up (above), down (under), to the left (right), in the middle of... Production of corresponding sentences with constant observation and verification of sentences.
-
Writing sentences after verification on the map. Example of such sentences translated into English: Puebla is in the center of Mexico. Chihuahua is above Durango...
-
Creation of maps working with real space and using memory (office, cabinet, home, garden).
-
Symbolic analysis of the Solar System. Observation and drawing of different concrete situations, use of models and schema. Use of oral questions: What is closer to the Sun: the Earth or Saturn? The Earth is between Venus and Mars.
-
Construction of objects by making models with matches. Constant verbal reflection and orientation on all aspects of the models, using all prepositions and spatial structures of the language (in Spanish).
-
Construction of models with the help of Kohs Cubes. Constant analysis of all spatial details of the models.
-
•Constant oral reflection. Usage of red and white squares at first. Usage of black and white models at the next stage.
STAGE 2
Objective: Rehabilitation of comprehension at the level of sentences without any support of concrete context.
Tasks:
-
Analysis of syntactic components of sentences: subject, predicate, and direct (indirect) object. Use of symbols and schemas for sentence construction and for each component of the sentence.
-
Analysis of texts (stories).
-
Patients production of her own compositions based on detailed analysis of spatial relations and word order.
STAGE 3
Objective: Rehabilitation of the ability to solve arithmetic problems. Constant usage of conceptual orientation and a schema for analyzing the problems was applied (Luria& Tsvetkova, 1979). Analysis of the semantic conditions in each problem: sufficient or insufficient elements for answering the problems final questions. Orientation for identifying the final and intermediate questions in the problem. Determination of the spatial direction of each operation: subtraction and division (to the left), sum and multiplication (to the right).
Tasks:
-
Simple problems with a direct grammatical structure (one operation)
-
Simple problems with an indirect (inverse) grammatical structure (one operation).
-
Complex problems with a direct structure (more than one operation).
-
Complex problems with an indirect structure (more than one operation).
-
Open problems which do not have solution. Such problems require more orientation and reflection from the patient.
Results of the Final Neuropsychological Assessment
Significant qualitative differences were observed in the final neuropsychological assessment. The patient was able to fulfill all constructive, perceptual, and written tasks. No semantic difficulties were observed in speech production. Writing and reading became accessible to the patient in all modalities. The members of the family and the patient herself could notice positive changes in the recall process for verbal information and in day-to-day organization of life.
Below are some examples of tasks presented to the patient during the final neuropsychological assessment:
Task: “Draw watches by instruction.”
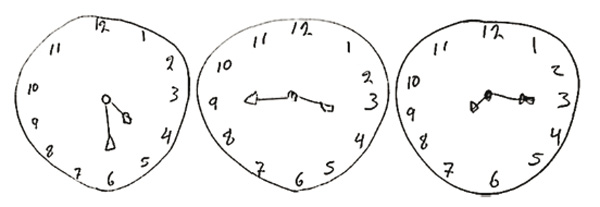
The patient had refused to fulfill this task before rehabilitation
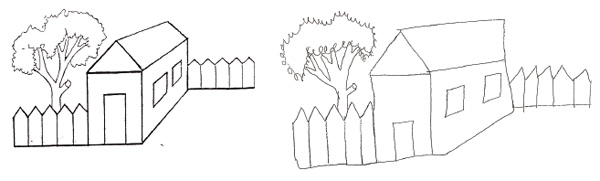
Task: Model of the house and its realization by the patient after rehabilitation. The patient had refused to fulfill this task before rehabilitation.
Task: Copy Rey figure
Task: Plan and writing composition for the patients chosen topic “My Weekend” (No translation into English is available.)
Discussion
It is practically impossible to find published neuropsychological studies of the syndrome of semantic aphasia in Spanish-speaking patients. Head (1926) was the first to use this designation. Similar kinds of semantic difficulties can be found in the literature, but in relation to other clinical pictures. For example, Leon-Carrion (2006) mentions patients who have lost spatial orientation after brain injury; these patients lost recognition of objects; forgot places and other people; and manifested confusion in their understanding of the time code and details of calendars. Other authors refer to semantic aphasia as speech difficulties, which include grammatical problems understanding spatial relations in passive phrases, subordinated phrases , and inverse constructions. Nevertheless, no studies on specific cases of patients which included early and final assessment, and implementation of rehabilitation programs, could be found (Benson & Ardila, 1996; Ardila & Ostrosky, 1991). In later publications, spatial difficulties were frequently presented without any reference to semantic aphasia; language and spatial orientation were presented in different chapters as isolated functions (Ostrosky & Ardila, 2010).
Our study shows the importance of elaborating original tasks for neuropsychological assessment according to the specific features of syntactic organization of each language (Spanish, in our case). We believe that it is no use to directly translate the items in neuropsychological tests for aphasia from other languages into Spanish. We insist on the necessity of a proper understanding and study of Luriasclassification of types of aphasia and the method for their identification (Luria,1999; Quintanar, 1999). Correct determination of the patients central difficulties permits the doctor to establish a precise diagnosis and, consequently, to prepare the content of the concrete tasks for neuropsychological rehabilitation.
Future neuropsychological studies might help the researcher get a precise clinical picture of semantic aphasia, and establish more kinds of typical difficulties of syntactic organization in the patients’ oral and writing production, and comprehension of speech. Our study doesn’t mention specific difficulties with word selection, and we consider that future work with the other clinical cases of patients with semantic aphasia would help researchers find out if this is really a problem in Spanish-speaking patients. It is also important to stress that similar clinical studies might be suggested for Spanish-speaking patients not only in Mexico, but also in other countries using the Spanish language.
In our study, the Program of Neuropsychological Rehabilitation was useful for the patient and has permitted her to re-establish functions of spatial orientation in verbal and non-verbal tasks and day-to-day life. We consider that the results obtained after application of the rehabilitation program allowed us to verify or to reject the hypothesis (what caused the alterations) on which the rehabilitation program was based. In other words, the success of the rehabilitation confirmed the neuropsychological diagnosis established during the initial assessment.
Our results show that the effectiveness of assessment directly leads to effectiveness of the whole process of elaboration and realization of rehabilitation. It is important to take into account the strong motivation on the level of the patient’s personality. We might add that the process of rehabilitation became a purpose of life for the patient during this joint activity (Frankl, 2013). Rehabilitation occurred as a shared activity between the psychologist and the patient, in which the patient was directed and oriented through all steps of the process. The final neuropsychological assessment pointed out significant qualitative evidence of improvement in spatial orientation and organization of information in all levels: material, perceptual, and verbal. The global and complex consideration of the clinical picture in cases of brain injury is more useful than the traditional separation of syndromes of aphasia, from problems of spatial orientation and tasks with building of blocks , which traditionally are more related to executive functions.
The tasks were always presented as actions, and not as simple exercises or training operations. This meant that the patient always knew at a conscious level the elements of the action: “what to do, why to do, and how to do.” The elements of “what to do” and “why to do” might be included as part of the motivational sphere of activity, and were essential for the whole process of rehabilitation. We might comment that the patient was afraid to work with Kohs Cubes at the beginning, but she was really happy and lit up a lot while achieving all the tasks at the end of her rehabilitation.
We might add that we also included “how to correct,” and we might say that the three functional parts of any human activity were represented in the program by “how to do”: orientation, execution, and verification (Galperin, 2009). External orientation was essential for the fulfillment of complex constructive tasks. The inclusion of different kinds of material, perceptual, and verbal tasks permitted us to follow the levels of formation of actions with spatial orientation, starting from the most concrete level, and passing up to a more general, abstract level (Talizina, 2009; Solovieva, 2014; Solovieva & Quintanar, 2016).
Conclusions
-
The neuropsychological syndrome of semantic aphasia can be established in Spanish-speaking patients.
-
Neuropsychological assessment and rehabilitation together make up a unique process.
-
Motivational support and intellectual involvement of the patients are fundamental for successful rehabilitation in adults.
-
External orientation and inclusion of self-consciousness for all operations with spatial orientation can be a useful strategy in cases of semantic aphasia.
References
Ardila, A. & Ostrosky, E (1991). Diagnostico del Dano Cerebral. Enfoque Neuropsicologico. [Diagnosis of Brain Damage. Neuropsychological Approach]. Mexico: Trillas.
Ardila, A. & Ostrosky, E (2011). Guta para el diagnostico neuropsicologico. [Guidence for Neuropsychological Diagnosis]. http://www.funlam.edu.co/modules/facultadpsicologia/item.php?itemid=877
Balasurbramanian, V. (2005). Dysgraphia in two forms of conduction aphasia. Brain and Cognition, 57, 8-15. doi: 10.1016/j.bandc.2004.08.012
Benson, D. & Ardila, A. (1996). Aphasia: A clinical perspective.New York: Oxford University
Press.
Boo, M. & Rose, M.L. (2011). The efficacy of repetition, semantic and gesture treatment for verb retrieval and use in Brocas aphasia. Aphasiology, 25, 2, 154-175. doi: 10.1080/02687031003743789
Cherney, L. R., Halper, A. S., Holland, A. L., & Cole, R. (2008). Computerized script for aphasia. Preliminary results. American Journal of Speech Language, 17, 19-34. doi: 10.1044/1058-
0360(2008/003)
Frankl, V. (1990). Mans Search for Meaning.Moscow: Progress.
Galperin, P.Ya. (2009). Tipos de orientacion у tipos de formacion de las acciones у los conceptos. [Types of orientation and types of formation of actions and concepts]. In: L. Quintanar & Yu.
Solovieva (Eds.) Las funciones psicologicas en el desarrollo del nino. [Psychologicla functions in childs development],76-79. Mexico: Trillas.
Glozman,}. (1999). Quantitative and qualitative integration of Lurian procedures. Neuropsychology Review, 9,1, 23-32. doi: 10.1023/A:1025638903874
Goodglass, H. 8c Kaplan, E. (1972). The assessment of aphasia and related disorders.Philadelphia: Lea & Febiger.
Goodglass, H., Kaplan, E., 8c Barresi, B. (1996). Test de Boston para el diagnostico de la afasia. [Boston test for diagnosis of aphasia]. Buenos Aires: Panamericana.
Harris, L., Olson, A., 8c Humphreys, G. (2014). The link between STM and sentence conprehension: A neuropsychological rehabilitation study. Neuropsychological Rehabilitation, 24, 5,
678-720. doi: 10.1080/09602011.2014.892885
Head, H. (1926). Aphasia and kindred disorders of speech.London: Cambridge University Press.
Hecaen, H. (1979). Aphasias. In: M.S. Gazzaniga (Ed.) Handbook behavioral neurobiology, vol. II: Neuropsychology. 239-289. New York: Plenum Press, doi: 10.1007/978-l-4613-3944-l_10
Kertesz, A. (1979). Aphasia and associated disorders.New York: Grune and Stratton.
Kiran, S., Des Roches, C, Villard, S., 8c Tripodis, Y. (2015). The effect of sentence comprehension treatment on a discourse comprehension in aphasia. Aphasiology, 29, 11, 1289-1311. doi:
10.1080/02687038.2014.997182
Kogan, V.M. (1962). The rehabilitation of language in aphasia.Moscow: Tsietin.
Lazaro, E., Quintanar, L., 8c Solovieva, Yu. (2010). Analisis neuropsicologico de pacientes con diferentes tipos de afasia. [Neuropsychological analysis of patients with different types of
aphasia]. Revista Neuropsicologia Latinoamericana.2,1, 33-46.
Leon-Carrion, J. (2006). Dano Cerebral. Una Guia para Familas у Terapeutas.[Brain Injury. Guidance for Families and Therapists].Madrid: Delta Publicaciones.
Leontiev, A.N. (1983). Selected psychological works. Moscow: Moscow State University.
Leontiev, D.A. (2011). Potential of personality: structure and diagnosis. Moscow: Sence.
Lopez, B. (2001). Orientaciones en rehabilitacion cognitiva [Orientations in cognitive rehabilita-
tion]. Revista de Neurologia,33,4, 383-387.
Luria, A.R. (1947). Traumatic Aphasia.Moscow: Academy of Medical Sciences.
Luria, A.R. (1964). Factors and forms of aphasia. In: A.V.S. De Reuck 8c M. O’Connor (Eds.)
Symposium on Disorders of Language.143-161. London: J. & A. Churchill Ltd. doi: 10.1002/9780470715321.ch9
Luria, A.R. (1972). A man with a shattered world.New York: Basic Books, Inc.
Luria, A.R. (1973). Fundamentals of neurolinguistics.Moscow: Moscow State University.
Luria, A.R., 8c Tsvetkova, L.S. (1979). La Resolucion de Problemas у sus alteraciones. [Resolution
of problems and their disturbances]. Barcelona: Fontanella.
Luria, A.R. (1999). Outline for the neuropsychological examination of patients with local brain lesions. Neuropsychology Review, 9,1, 9-22. doi: 10.1023/A:1025686819804
Marini, A., Caltagirone, C., Pasqualetti, R, 8c Carlomagno, S. (2007). Patterns of language improvement in adults with non-chronic non-fluent aphasia after specific therapies. Aphasio-
logy, 21, 139-163. doi: 10.1080/02687030600633799
Moreno, P. & Blanco, C. (2000). Hacia una teoria comprensiva de la rehabilitacion de funciones cerebrales como base de los programas de rehabilitacion en enfermos con dano cerebral.
[About the comprehensive theory of rehabilitation of brain functions as the basis for programs of rehabilitation of patients with brain injury]. Revista de Neurologia, 30, 8, 779-783.
Ostrosky, F. & Ardila, A. (2010). Cerebro у lenguaje. [Brain and Language].Mexico: Trillas.
Pena-Casanova, J. (2005). Test Barcelona-R: Teona e interpretacion. [Test Barcelona-R: Theory
and Interpretation]. Barcelona: Masson.
Pulvermuller, R & Berthier, M. L. (2008). Aphasia therapy on a neuroscience basis. Aphasiology, 22, 6, 563-599. doi: 10.1080/02687030701612213
Quintanar, L. (1999). Modelos neuropsicologicos en afasiologia. [Neuropsychological Models of
Aphasia]. Mexico: Puebla Autonomous University.
Quintanar, L. & Solovieva, Yu. (2001). Metodos de Rehabilitacion en la Neuropsicologia del Adulto. [Methods of Rehabilitation in Neuropsychology of Adults].Mexico: Puebla Autonomous University.
Quintanar, L. & Solovieva, Yu. (2002). Analisis neuropsicologico de las alteraciones del lenguaje. [Neuropsychological Analysis of speech disturbances]. Revista de Psicologia General у Aplicada, 55,1, 67-87.
Quintanar L., Solovieva, Yu., & Lazaro E. (2010). Neuropsychological challenges of assessment of
Spanish-speaking patients.1,1-9. IBIA, Brain Injury.
Quintanar, L., Lazaro, E., & Solovieva, Yu. (2009). La rehabilitacion neuropsicologica a traves
de la reorganization de los sistemas funcionales. [Neuropsychological Rehabilitation by reorganization of functional systems].In: E.A. Escotto, M. Perez у M.A. Villa (Eds.) Desarrolloу alteraciones del lenguaje, neuropsicologia у genetica de la inteligencia. [Development and disturbances of speech],249-273. Mexico: UNAM.
Quintanar, L., Solovieva, Yu., & Leon-Carrion, J. (2011). Evaluacion Clinica Neuropsicologica de la Afasia Puebla-Sevilla. [Clinical Neuropsychological Assessment of Aphasia Puebla-Sevilla].Mexico: Puebla Autonomous University.
Quintanar, L. & Solovieva, Yu. (2013). Evaluacion neuropsicologica breve para adultos. [Brief Neuropsychological Assessment of Adults]. Mexico: Puebla Autonomous University.
Quintanar, L. & Solovieva, Yu. (2016). Rehabilitacion neuropsicologica. Historia, teoriaу practica.
[Neuropsychological Rehabilitation. History, theory and practice]. Mexico: Puebla Autonomous University.
Rasquin, S.M.C., Welter, J., & Van Heugten, C.M. (2013). Course of cognitive functioning during stroke rehabilitation. Neuropsychological Rehabilitation,23, 6, 811-823. doi:
10.1080/09602011.2013.821950
Smeets, S.M.J., Vink, M., Ponds, R.W., Winkens, L., & Van Heugten, C.M. (2017). Changes in impaired self-awareness after acquired brain injury in patients following intensive neuropsychological rehabilitation. Neuropsychological Rehabilitation,27, 1, 116-132. doi: 10.1080/09602011.2015.1077144
Solovieva, Yu. (2014). La actividad intelectual en el paradigma historico-cultural. [Intellectual
Activity in the historical and cultural paradigm]. Mexico: Ediciones CEIDE.
Solovieva, Yu., Chavez, M., & Quintanar, L. (2001). Alteraciones de la actividad intelectual en pacientes con afasia semantica. [Impairments of Intellectual Activity in Patients with Seman-
tic Aphasia]. Revista Espanola de Neuropsicologia,3, 2,12-33.
Solovieva, Yu., Renteria, E, & Quintanar, L. (2001). Evaluacion у rehabilitacion de la actividad intelectual en un caso de la afasia semantica. [Assessment and Rehabilitation of Intellectual
Activity in Patients with Semantic Aphasia].In: L. Quintanar & Yu. Solovieva (Eds.) Metodos de rehabilitacion en la neuropsicologia del adulto. [Methods of Rehabilitation in the Neuropsychology of Adults], 189-224. Mexico: Puebla Autonomous University.
Solovieva, Yu., Villegas, N., Jimenez, R, Orozco, M., & Quintanar, L. (2001). Alteraciones de la
esfera afectivo-emocional en diferentes tipos de afasia. [Impairments of the Affective-Emotional Sphere in Patients with Different Types of Aphasia]. Cuadernos hispanoamericanos de psicologia, 1 (2), 63-74.
Solovieva, Yu. & Quintanar, L. (2016). The role of the zone of proximate development in interactive assessment of intellectual development. British Journal of Education, Society & Behav-
ioural Science. 14 (1), 1-11.
Talizina, N.E (2009). La teoria de la actividad aplicada a la ensenanza. [Activity Therapy Applied to Teaching]. Mexico: Puebla Autonomous University.
Tsvetkova, L. (1977). Reeducacion del lenguaje, la lectura у la escritura. [Re-education of language, reading and writing]. Barcelona: Fontanella.
Tsvetkova, L. (1988). Aphasia and rehabilitation education. Moscow: Education.
To cite this article: Solovieva Yu., Quintanar L. (2018). Rehabilitation of semantic aphasia in spanish speaking patient. Psychology in Russia: State of the Art, 11 (1), 137-150.
The journal content is licensed with CC BY-NC “Attribution-NonCommercial” Creative Commons license.







