Sense of humor disorders in patients with schizophrenia and affective disorders
Enikolopov, Sergey N.  Mental Health Research Center, Russian Academy of Medical Sciences, Moscow, Russia
Mental Health Research Center, Russian Academy of Medical Sciences, Moscow, Russia
Abstract
The article presents an empirical study of sense of humor disorders in patients with schizophrenia and affective disorders. Several parameters of analysis are distinguished: humor recognition, humor preferences and the level of laughing activity. It is showed that patients with schizophrenia are characterized by inability to recognize humor. As soon as patients with schizotypal disorder do recognize humor, this may be used as a diagnostic criterion in clinical practice. Sense of humor in patients with schizophrenia and affective disorders acquires peculiarities which are defined here as preferences of certain cognitive mechanisms and topics of jokes.
Received: 23.12.2013
Accepted: 10.03.2014
Themes: Clinical psychology
PDF: http://psychologyinrussia.com/volumes/pdf/2014_1/2014_1_146-157.Pdf
Pages: 146-157
DOI: 10.11621/pir.2014.0114
Keywords: sense of humor, humor recognition, schizophrenia, schizotypal disorder, affective disorder
Introduction
Nowadays humor research in psychology becomes more and more popular. Humor is a kind of universal phenomenon and is connected with all spheres of human being and social functioning (Ivanova, Enikolopov, 2006; Martin, 2007). Many clinicians suggest sense of humor disorder to be an important diagnostic criterion. Thus Arieti (1950, as cited in Forabosco, 2007) called schizotypal intellectual disorder “paleological thinking” and supposed it to be connected with humor impairment. The similar idea was declared by Levin (1957, as cited in Forabosco, 2007). That’s why sense of humor study in psychiatric patients is of present interest. Sense of humor is such a unique psychic phenomenon that reveals the unit of intellect and affect. So, some clinicians suppose its disorder to appear even earlier than more severe intellectual or emotional disorders (Luk, 1977). If to confirm this, the possibility of early diagnostics would exist. Despite of its practical meaning, there is quite a few empirical data on humor in clinical context. So, this study becomes one of the first steps on the way to overcome this gap.
The existing studies on sense of humor disorders may be combined into two main approaches: quantitative and qualitative (Ivanova, Enikolopov, 2009; Forabosco, 2007). The quantitative one supposes sense of humor “decrease” in psychiatric patients (e.g., Levine, Abelson, 1969; Levine, Redlich, 1955). The approach doesn’t give convincing explanation of such kind of deficit and doesn’t allow to distinguish patients with different diagnoses. Moreover, sense of humor is a complex multidimensional phenomenon (see Martin, 2007; Ruch, 2007) and includes a list of parameters: intellectual understanding of punch line, emotional involvement, disposition to laughter etc. Evidently, sense of humor disorder also includes different components.
The second, qualitative approach is connected with analysis of sense of humor peculiarities in patients with different psychiatric syndromes (Polimeni, Reiss, 2006; Polimeni et al., 2010; Werth, Perkins, Boucher, 2001). Forabosco (2007) supposes that psychopathology doesn’t simply decrease humor but rather various diagnostic categories may be accompanied by a specific picture of humor alteration. This approach gives much more possibilities for conceptualizing, but it hasn’t gone further than description of the specifics yet. This study is made mostly in the flow of qualitative approach but at the same time includes the analysis of sense of humor components that may decrease.
The main hypothesis is that sense of humor disorders have nosological specifics in patients with schizophrenia and affective disorders. For affective disorders we suggest to reveal the decrease of emotional and behavioral response (laughter) while intact intellectual understanding of punch line. As for schizophrenic patients the stress was done more to a cognitive deficit in humor recognition and revealing specific “schizotypal” humor preferences. So, the two mental deceases were taken as characterized with the opposite sense of humor disorders.
Method
Research participants
The four groups of subjects took part in the study. All of them were young males from 17 to 32 years old (mean age of 22), totally 101 subjects. The first group contains patients with affective disorders such as manic-depressive syndrome and cyclothymia — F-31, F-33, F-34 according to ICD-10 (18 subjects). It includes both depressive and manic ones. The second group is composed of patients with schizotypal disorder — F-21.0 (23 subjects). These subjects are characterized by schizotypal intellectual disorders without psychotic symptoms. The third group includes patients with schizophrenia and schizoaffective disorders which are characterized by such psychotic symptoms as delusions and hallucinations — F-20, F-25 (30 subjects). And the fourth is control group of healthy people (30 subjects).
Instruments
Several levels of analysis were distinguished for sense of humor disorder: 1) humor recognition, 2) subjective assessment of jokes — humor preferences and 3) the degree of behavioral response (laughter).
The method of humorous phrases distinguishing was elaborated to study an ability to recognize humor among serious information (Ivanova et al., 2008a). It includes 17 phrases presented on separate sheets of paper and mixed: humorous, nonhumorous and witty aphorisms. The subjects were to distinguish humorous phrases. The deviation from assessments of the control group was taken as a disorder of humor recognition. Taking into account an earlier study (Ivanova et al., 2005) it was hypothesized that the ability to recognize humor decreases in patients with schizophrenia.
The assessing of humor preferences method was designed to study preferable cognitive mechanisms of jokes (Ivanova et al., 2008b). It includes 36 verbal jokes each based on one of the 12 cognitive mechanisms defined by Russian psychologist Luk: false opposition (pseudocontrast), false intensifying, absurd, nonsense, mixing of different styles or combining different plans, hint, ambiguity, irony, metaphor litteralization (reversed comparison), comparison on unimportant attribute, repetition, paradox (Luk, 1968; 1977). The subjects were to divide jokes into 4 categories: 1) the worst, 2) not funny, 3) funny, 4) the best. Thus each joke got a score from 1 to 4.
While a subject was doing the task, an experimenter noted the jokes familiar to the subject and his laughing response: 0 — no reaction, 1 — smile, 2 — sneering, 3 — laughter, 4 — burst of laughter. Subjects were also to choose the 2 worst and the 2 best jokes which were discussed then. In the discussion a subject was asked which character of the joke he tended to identify with reading the joke. In the early study it was revealed that patients with schizophrenia and affective disorders tend to identify with the mocked character of a joke, and do it twice more often than healthy people (Ivanova et al., 2005).
In this study it was suggested to confirm the previous data. The identifications with the mocked character were assessed from 0 — not a single in 4 jokes to 4 — in all 4 jokes.
A number of standard methods were used to assess cognitive and emotional disorders in the patients. Schizotypal intellectual disorder such as inability to filter out irrelevant stimuli was revealed with such tests as objects classification and excluding irrelevant object (Zeigarnik, 1972). The degree of intellectual disorder was assessed as 0 — no disorder, 1 — light disorder (single mistakes), 2 — severe disorder (inability to filter out irrelevant stimuli). Depressive syndrome was measured by the Beck Depression Inventory (BDI) (Beck et al., 1961; Beck, Steer, Garbin, 1988). Projective draw of unreal animal was used to reveal aggression and paranoiac tendencies.
Results
Humor recognition
The T-criterion analysis was done to reveal which phrases of the set were taken as humorous, nonhumorous and differently.
Table 1 demonstrates that all subjects assessed phrases the same way with high significance except the patients with schizophrenia. So, the ability to distinguish humor decreases under this mental decease. The disorder may be presented either as an inability to recognize humor (the patients didn’t feel humor in phrases No 1 and 7), or as a tendency to inject humorous sense into nonhumorous text (they suppose serious aphorism No16 to be a joke) (р<0.001).
Table 1. Group assessments of phrases as humorous/nonhumorous/differently р<0.001.
Group |
N |
Phrases assessed as humorous |
Phrases assessed as nonhumorous |
Phrases assessed differently |
Control |
30 |
1, 3, 5, 7, 11, 12 |
2, 4, 8, 13, 14, 15, 16, 17 |
6, 9, 10 |
Affective dis. |
18 |
1, 3, 5, 7, 11, 12 |
2, 4, 8, 13, 14, 15, 16, 17 |
6, 9, 10 |
Schizotypal dis. |
23 |
1, 3, 5, 7, 11, 12 |
2, 4, 8, 13, 14, 15, 16, 17 |
6, 9, 10 |
Schizophrenia |
30 |
3, 5, 11, 12 |
2, 4, 8, 13, 14, 15, 17 |
1, 6, 7, 9, 10, 16 |
In order to connect the deviation of phrases assessments (in comparison to the control group) and intellectual disorder the oneway ANOVA was used. Intellectual disorder (0 — no disorder, 1 — light disorder, 2 — severe disorder as inability to filter out irrelevant stimuli) was taken as an independent variable. As a dependent variable the deviation of phrases assessments was taken, which was counted by the following formula:
![]()
ni — mean assessment of the phrase i in the control group (humorous/nonhumorous), ai — assessment of the phrase i by subject а, wi = 1/σi, i varies from 1 to 17.
The results demonstrate that the more degree of intellectual disorder has a subject the more his assessments deviate from the control group ones (Figure 1, p<0.05).
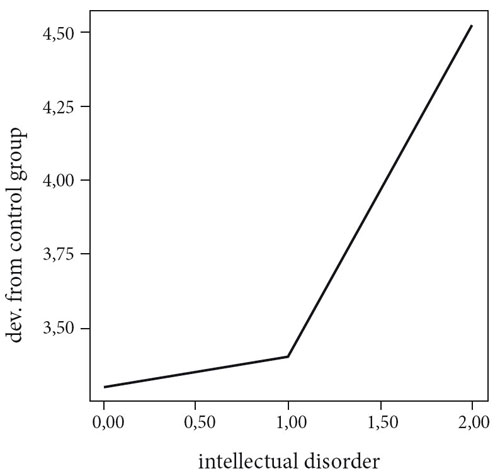
Figure 1. Connection between the degree of intellectual disorder and assessments’ deviation of phrases from the control group
Interestingly the deviation is low for the subjects with light intellectual disorder and high in patients with severe cognitive deficit. So, the difference of phrases assessments between the patients with schizophrenia and the other subjects may be explained by schizotypal inability to filter out irrelevant stimuli.
As expected, there is no significant correlation between depressive syndrome and deviation of phrases assessments. This fact is consistent to clinical observations. Depressive patients do not feel like to joke, although having no cognitive impairments they easily recognize humor and sometimes appreciate it (for ex. Forabosco, 2007).
Laughing activity
The analysis of behavioral responses to the jokes shows group differences on laughing activity (Figure 2).
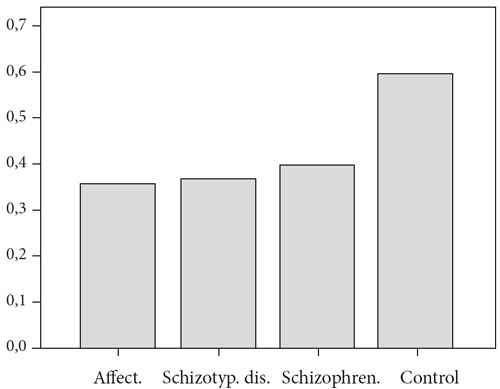
Figure 2. Group differences in laughing activity
The laughing activity is significantly higher in the control group than in all others (T-criterion, р<0.001). The differences between the groups of patients are nonsignificant. Nonetheless laughing activity is the lowest in patients with affective disorders, almost equal in patients with schizotypal disorder and higher in the patients with schizophrenia. This tendency may be explained by emotional disorder. The more depressive component defines the mental state the lower the degree of laughing activity is. The statement is confirmed by negative correlation between laughing activity and the degree of depression according to BDI (r=-0.22р<0.05).
The covariance between jokes assessments and laughing responses is significantly higher in the control group in comparison to all others (T-criterion, р<0.001). It shows natural response of healthy people to good humor — laughter, in comparison with more disconnected activity of patients. The differences in the three experimental groups are not significant.
Preferable cognitive mechanisms
Humor based on mixing different styles, which is putting the situation into unrelevant context, arouse higher laughing response in patients with affective disorders (means comparison by T-criterion, р≤0.01). For example: “Vasilisa the Beautiful got married with Ivan the Fool and became Vasilisa the Fool”, “50 gramms of investments and I’m immovable”.
Patients with schizophrenia, in comparison with the others, expressed higher laughing response to the jokes based on paradox (р≤0.01) when some deep meaning is found in seemingly meaningless words. For example: “The closer you make the acquaintance of a person the farther you wish to send him away”.
The analysis of jokes assessments shows that patients with schizophrenia also tend to prefer humor based on comparison by latent attribute (р≤0.1). For example: “— What is the difference between women and mosquitoes? — Mosquitoes only bother you in the summertime”.
The analysis of topics
Besides cognitive mechanisms, the topics of jokes were taken into account. The following topics were supposed to have an influence on jokes assessments: 1) sex, 2) illness, 3) death, 4) alcoholism and drug addiction. The method of structural equation modeling (Bentler, 1995) allowed to establish statistical significance of the topics and their preferences in the groups of subjects. 17 jokes from the general set that contained the topics (latent factors) were taken as measured variables. Nosological groups and psychiatric syndromes were seen as determinants of the topics’ preferences/rejections. The data was analyzed using EQS software. χ2 = 191, df=198, р=0,623, CFI=1, RMSEA=0.
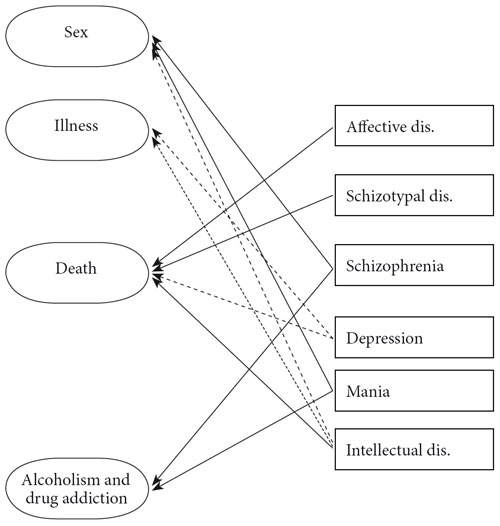
Figure 3. Preferences and rejections of humor topics
The meanings demonstrate accordance between the model and the experimental data. Figure 3 shows the obtained determinations. Correlations between residuals (E) and correlations between predictors (independent observed variables) are missed on the schema. Solid arrows present positive determinations, dotted — negative. Bold arrows are used for connections with significance H0<0.05 two-tailed criterion, ordinary arrows are used for connections with significance H0<0,05 one-tailed criterion.
The following tendencies may be noted. Patients with depressive syndrome reject jokes about illness and death. For example: “Vovochka, don’t hit the boy on his head with a spade, otherwise you may sweat and catch a cold”, “Doctor to his patient:
— I have bad news for you... — Doctor, will I die? — No, we are going to treat you.”, “She was very well put together, although her right hand was sticking out of the suitcase”.
On the contrary, patients with intellectual disorder prefer these jokes but reject sexual humor. For example: “Two condoms talking: — I’ve heard they want to use us... — Come on! We’ll break through”.
Patients with schizophrenia and manic syndrome prefer sexual humor and jokes about alcoholism and drug addiction. For example: “— Say “No” to drugs! — “No” say to drugs! — And stop talking to drugs at all!”, “50 gramms of investments and I’m immovable”.
Familiar jokes
During the experimental procedure the number of jokes familiar to the subject was noted. It was hypothesized that patients with schizophrenia like humor less and use it rarely, so know less jokes than healthy people. To verify the suggestion we compared means for two independent samples by T-criterion. The results confirm the hypothesis. The number of familiar jokes from the given set was higher for subjects of the control group than for the patients with schizotypal disorder and schizophrenia (р<0.001). The difference between patients with affective disorder and healthy subjects was nonsignificant.
Figure 4. Connection between the degree of intellectual disorder and mean number of jokes familiar to subjects
Oneway ANOVA gave negative connection between the mean number of jokes familiar to a subject and the degree of his intellectual disorder (Figure 4, р≤0.001).
Identification with the mocked character
The data obtained in our early study showed that one of the mechanisms of sense of humor disorder is a tendency to identify with the mocked character of a joke (Ivanova et al., 2005). In this study it was planned to make more detailed analysis of the phenomenon. The discussion of the 2 worst and the 2 best jokes included such a question as which character’s point of view a subject takes while reading jokes. The number of identifications with the mocked character varied from 0 to 4 (0 — not a single joke from the four, 4 — all 4 jokes). Surprisingly, the results don’t confirm the early data. The mean number of such identifications was higher for experimental groups than for the control but nonsignificantly.
Discussion
The study demonstrates that sense of humor is a complex, multidimensional function. So, sense of humor disorder may also touch different levels. The most severe one is inability to recognize humor. Then we described a decrease of laughing response and pathological changes in types of humor preferences revealed by preferable cognitive mechanism and topic.
The difficulties in humor recognition characterize patients with schizophrenia and this is consistent to the data of the early study (Ivanova et al., 2005). The inability to recognize humor in these patients is connected with schizotypal intellectual disorder that is impossibility to filter out irrelevant stimuli. It’s important that light intellectual disorder revealed as making single mistakes in diagnostic tests don’t lead to such inability. That is why humor recognition may be seen as a useful diagnostic tool to divide schizotypal disorder and schizophrenia in clinical practice.
Affective disorders lead to decrease of general laughing activity. Nonetheless the group differences are not so clear. This may be interpreted several ways. First of all, depressive syndrome was observed not only in affective disorder group but also in some patients with schizophrenia. Second, the decrease of laughing response in all patients in comparison with the control group may be connected with the very fact of illness and being in hospital. The negative emotions may not reach the degree of clinical depression, but still may have an influence.
Observing the way how patients behave during the procedure led to the following hypothesis. Healthy people usually assess positively the jokes they laugh at and vice versa. Whereas patients with mental disorders often assess jokes independently on their laughing response. The group differences in covariances between jokes assessments and laughing responses confirm the clinical observations.
The covariance between jokes assessments and laughing responses is significantly higher in the control group in comparison to all others. The differences in the three experimental groups are not significant. Speaking about depressive patients, the dissociation may be explained by the decrease of laughing activity. On the other hand, schizophrenic patients may hide their positive assessment of jokes with some topics because of paranoiac tendencies.
The analysis of sense of humor nosological specifics based on cognitive mechanisms allows to reveal only some tendencies which demand further confirmation. This may be connected either with lack of strictness of the typology, or difficulty to define cognitive mechanism of concrete jokes, or co-existing of several cognitive mechanisms in one joke. Nonetheless, it may be said definitely that Luk’s cognitive mechanisms don’t have equal meaning for describing pathological sense of humor.
The jokes based on mixing different styles increase laughing activity in patients with affective disorders. The essence of the cognitive mechanism is the opposition between the style and the content of joke and it may be associated with clinical symptom of affective disorders that is easy shift from one polar state to another.
Patients with schizophrenia prefer humor based on comparison by latent attribute. The essence of the cognitive mechanism is taking together things which are absolutely heterogeneous. This is also known as overinclusiveness and defines schizotypal inability to filter out irrelevant stimuli. Interestingly, jokes based on comparison by latent attribute don’t increase laughing response in these patients. So, it seems to be more of aesthetical delight.
Patients with schizophrenia express higher laughing response to the jokes based on paradox. When distinguishing humorous phrases these patients often took humorously the serious aphorism also based on paradox. Luk describes the essence of the cognitive mechanism the following way. The usual expressions seem to be replaced insignificantly. As a result the meaning changes to the opposite and the whole becomes to be nonsense. But it is still possible to make sense of this nonsense, find new deep meaning (Luk, 1968). It is important to note that the tendency to “make sense of nonsense” is one of the main characteristics of schizotypal speech. Apparently, comparison by latent attribute and paradox are the cognitive mechanisms that show schizotypal sense of humor described by clinicians.
The assessment of a joke depends also on its topic. The results of this analysis are discussible. There’s a need to confirm them in further research with a specially elaborated method. Nonetheless, several connections seem to be clear. Patients with depressive syndrome reject jokes about illness and death which may be too painful for them. This contradicts to the data of Goldsmith (1984) who obtained positive correlation between the suicidal severety and preference of humor about death (as cited in Forabosco, 2007). Patients with schizophrenia and manic syndrome prefer sexual humor and jokes about alcoholism and drug addiction. This may be referred to decrease of criticism in these patients which may lead to deviant psychopathic behavior.
The data obtained on the number of jokes familiar to subjects also shows group differences. Healthy people, as well as patients with affective disorders, know and remember much more jokes than patients with schizophrenia. In case of “pure” depression sense of humor changes temporarily. During remission stage positive attitude to humor recovers. On the contrary, sense of humor in schizophrenia reveals more stable pathological features.
The number of familiar jokes significantly correlates with intellectual disorder. The more the degree of intellectual disorder the more difficult for the patient is to understand humor. This leads to negative attitude to humor in general, increase of autism and decrease of motivation to remember jokes.
The data obtained on the tendency to identify with the mocked character is not clear. No significant group differences were obtained what contradicts to the early data (Ivanova et al., 2005). In comparison with this study, the previous one had smaller sample of subjects, but larger set of jokes (10 jokes instead of 4 in this study). That could give higher reliability of the measure. Also it is possible that patients with paranoiac syndrome avoid extreme assessments of jokes provocating identifications with the mocked character.
Here’s an example of such identification. Patient with schizophrenia discusses the joke No31 (Workers are needed to work on a work. The salary is money). The subject says he reads it as if he was a person who gives the announcement. Then he explains that he could give such an announcement “only if he was an idiot”. That’s why the joke annoyed him and he chose it as one of the worst.
The phenomenon of identification with the mocked character is close to the syndrome of gelotophobia or pathological fear to be laughed at described by Titze and Ruch. (Ruch, 2009; Ruch, Proyer, 2008a,b). According to Ruch and Proyer (2008a,b), patients with this syndrome tend to interpret uncertain situations of laughter as mockery.
Conclusion
To conclude, psychiatric patients do have sense of humor, but it may be altered in comparison with the controls on different parameters such as humor recognition, humor preferences (cognitive mechanisms and topics of jokes), laughing activity and may be others. Such a sense of humor alteration depends on nosology and may be used in clinical diagnostics. Thus patients with schizophrenia have humor recognition disorder in comparison with the controls.
Acknowledgements
Our gratitude goes to all the subjects who participated in the study and were very helpful discussing their attitude towards jokes. We appreciate the help of medical stuff of Scientific Center for Mental Health of RAMS. The first author is especially thankful to Drs Willibald Ruch and Giovannantonio Forabosco who gave very useful advices and emotional support in preparation of the English version of the article.
The study was supported by the Russian Humanitarian Science Foundation. Grant No13-06-00024.
References
Beck, A.T., Ward, C.H., Mendelson, M., Mock, J., & Erbaugh, J. (1961). An inventory for measuring depression. Archives of General Psychiatry 4, 561-571. doi: 10.1001/archpsyc.1961. 01710120031004
Beck, A.T., Steer, R.A., & Garbin, M.G. (1988). Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clinical Psychology Review 8(1), 77–100. doi:10.1016/0272-7358(88)90050-5
Bentler, P.M. (1995). EQS Structural Equations Program Manual. CA, Encino: Multivariate Software, Inc.
Forabosco, G. (2007). The ill side of humor: Pathological conditions and sense of humor. In W. Ruch (Ed.), The Sense of Humor: explorations of a personality characteristic(pp. 271– 292). New York: Mouton de Gruyter.
Ivanova, E.M., & Enikolopov, S.N. (2006). Issledovanija chuvstva umora v psyhologii (obzor) [The sense of humor research in psychology (review)]. Voprosi psyhologii [Issues in Psychology], 4, 122–133.
Ivanova, E.M., & Enikolopov, S.N. (2009). Psyhopatologija i chuvstvo umora [Psychopathology and sense of humor]. Sovremennaya terapya psyhicheskih rasstrojstv [Contemporary Therapy of Mental Disorders], 1, 19–24.
Ivanova, E.M., Enikolopov, S.N., & Maximova, M.U. (2005). Psyhologicheskie mehanismi narushenia chuvstva umora pri schizophrenii i cyclothymii [Psychological mechanisms of sense of humor disorder under schizophrenia and cyclothymia]. Psyhiatrija [Psychiarty], 3, 60–65.
Ivanova, A.M., Enikolopov, S.N., & Mitina, O.V. (2008a). Narushenie raspoznavanya umora u bol’nyh schizofreniej [Humor recognition in patients with schizophrenia]. Voprosi psyhologii [Issues in Psychology], 6, 75–81.
Ivanova, A.M., Enikolopov, S.N., & Mitina, O.V. (2008b). Narushenija chuvstva umora pri schizophrenii I affectivnyh rasstrojstvah [Humor preferences in psychiatric patients]. Voprosi psyhologii [Issues in Psychology], 1, 45–57.
Levine, J., & Abelson, R. (1969). Humor as a Disturbing Stimulus. In J. Levine (Ed.) Motivation in Humor. New York: Atherton Press.
Levine, J., & Redlich F.C. (1955). Failure to understand humor. Psychoanalytic Quarterly, 24, 560–572.
Luk, A.N. (1968). O chuvstve umora i ostroumii [On sense of humor and wit]. Moscow: Iskusstvo.
Luk, A. N. (1977). Umor, ostroumie, tvorchestvo. [Humor, wit, creativity]. Moscow: Iskusstvo.
Martin, R.A. (2007). The psychology of humor: An integrative approach. Burlington. MA: Elsevier Academic Press.
Polimeni, J., & Reiss, J.P. (2006). Humor perception deficits in schizophrenia. Psychiatry Research, 141, 229–232. doi: 10.1016/j.psychres.2005.05.012
Polimeni, J.O., Campbell, D.W., Gill, D., Sawatzky, B.L., & Reiss, J.P. (2010). Diminished humourperception in schizophrenia: relationship to social and cognitive functioning. Journal of psychiatry research, 44(7), 434–440. doi: 10.1016/j.jpsychires.2009.10.003
Ruch, W. (Ed.) (2007). The Sense of Humor: explorations of a personality characteristic. New York: Mouton de Gruyter.
Ruch, W. (2009). Fearing humor? Gelotophobia: The fear of being laughed at Introduction andoverview. Humor: International Journal of Humor Research, 22(1/2), 1–26. doi: 10.1515/ HUMR.2009.001
Ruch, W., & Proyer, R.T. (2008a). The fear of being laughed at: Individual and group differences in Gelotophobia. Humor: International Journal of Humor Research, 21(1), 47–67. doi: 10.1515/HUMOR.2008.002
Ruch, W., & Proyer, R.T. (2008b). Who is gelotophobic? Assessment criteria for the fear of being laughed at. Swiss Journal of Psychology, 67(1), 19–27. doi: 10.1024/1421-0185.67.1.19
Werth, A., Perkins, M., & Boucher, J. (2001). Here’s the weavery looming up. Autism, 5(2), 111– 125. doi: 10.1177/1362361301005002002
Zeigarnik, B. (1972). Experimental abnormal psychology. New York: Plenum Press. doi: 10.1007/ 978-1-4684-7421-3
To cite this article: Ivanova A.N., Enikolopov S.N., Mitina O.V. Sense of humor disorders in patients with schizophrenia and affective disorders. Psychology in Russia: State of the Art, 7(1), 146-157.
The journal content is licensed with CC BY-NC “Attribution-NonCommercial” Creative Commons license.







